

A comprehensive overview of medical error in hospitals using incident-reporting systems, patient complaints and chart review of inpatient deaths
- PMID: 22359567
- PMCID: PMC3281055
- DOI: 10.1371/journal.pone.0031125
A comprehensive overview of medical error in hospitals using incident-reporting systems, patient complaints and chart review of inpatient deaths
Abstract
Background: Incident reporting systems (IRS) are used to identify medical errors in order to learn from mistakes and improve patient safety in hospitals. However, IRS contain only a small fraction of occurring incidents. A more comprehensive overview of medical error in hospitals may be obtained by combining information from multiple sources. The WHO has developed the International Classification for Patient Safety (ICPS) in order to enable comparison of incident reports from different sources and institutions.
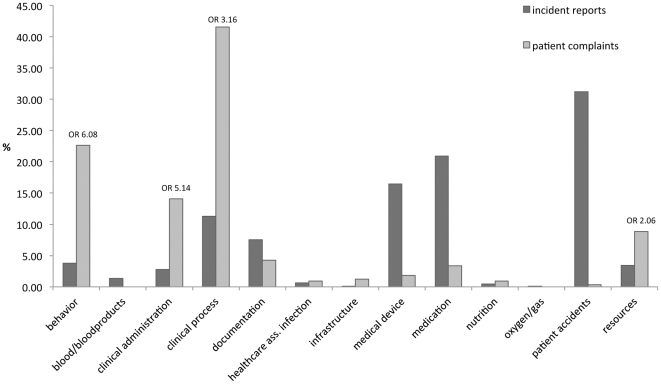
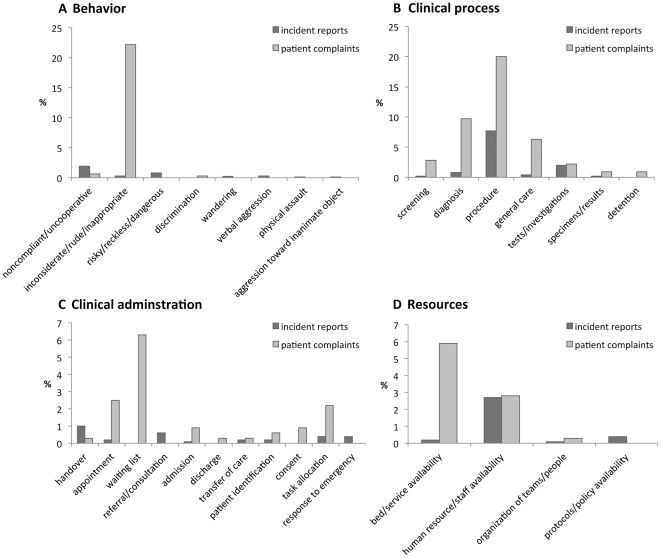
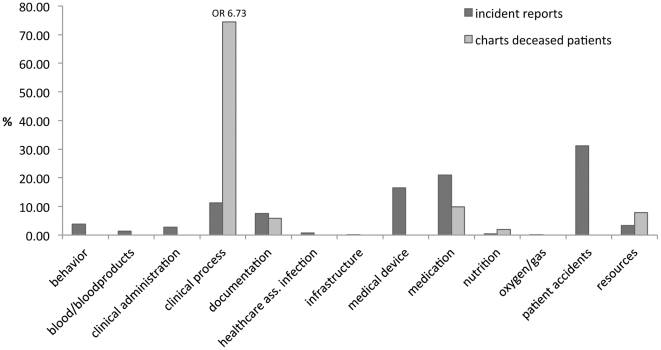
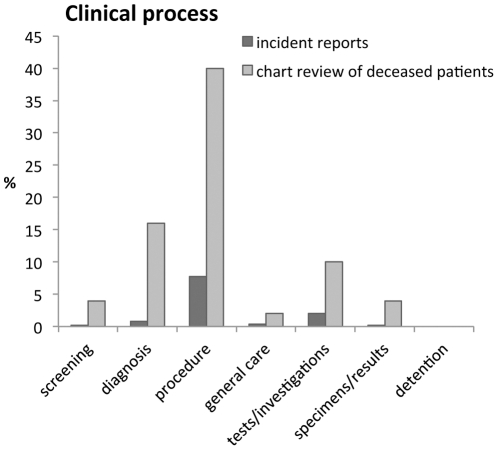
Methods: The aim of this paper was to provide a more comprehensive overview of medical error in hospitals using a combination of different information sources. Incident reports collected from IRS, patient complaints and retrospective chart review in an academic acute care hospital were classified using the ICPS. The main outcome measures were distribution of incidents over the thirteen categories of the ICPS classifier "Incident type", described as odds ratios (OR) and proportional similarity indices (PSI).
Results: A total of 1012 incidents resulted in 1282 classified items. Large differences between data from IRS and patient complaints (PSI = 0.32) and from IRS and retrospective chart review (PSI = 0.31) were mainly attributable to behaviour (OR = 6.08), clinical administration (OR = 5.14), clinical process (OR = 6.73) and resources (OR = 2.06).
Conclusions: IRS do not capture all incidents in hospitals and should be combined with complementary information about diagnostic error and delayed treatment from patient complaints and retrospective chart review. Since incidents that are not recorded in IRS do not lead to remedial and preventive action in response to IRS reports, healthcare centres that have access to different incident detection methods should harness information from all sources to improve patient safety.
Conflict of interest statement
Figures
References
-
- Brennan TA, Leape LL, Laird NM, Hebert L, Localio AR, et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. New England Journal of Medicine. 1991;324:370–376. - PubMed
-
- Kohn KT, Corrigan JM, Donaldson MS. To err is human. Building a safer health system. Washington, DC: National Academy Press; 1999. - PubMed
-
- Hutchinson A, Young TA, Cooper KL, McIntosh A, Karnon JD, et al. Trends in healthcare incident reporting and relationship to safety and quality data in acute hospitals: results from the National Reporting and Learning System. Qual Saf Health Care. 2009;18:5–10. - PubMed
-
- Jones KJ, Cochran G, Hicks RW, Mueller KJ. Translating Research Into Practice: Voluntary Reporting of Medication Errors in Critical Access Hospitals. The Journal of Rural Health. 2004;20:335–343. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
