

Multiple biomarkers for risk prediction in chronic heart failure
- PMID: 22361079
- PMCID: PMC3387487
- DOI: 10.1161/CIRCHEARTFAILURE.111.965020
Multiple biomarkers for risk prediction in chronic heart failure
Abstract
Background: Prior studies have suggested using a panel of biomarkers that measure diverse biological processes as a prognostic tool in chronic heart failure. Whether this approach improves risk prediction beyond clinical evaluation is unknown.
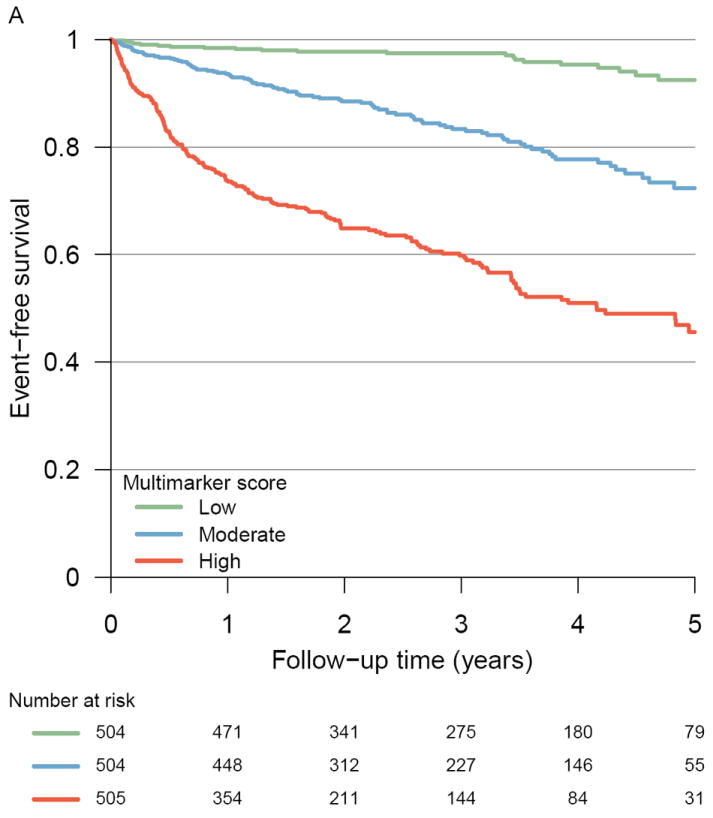
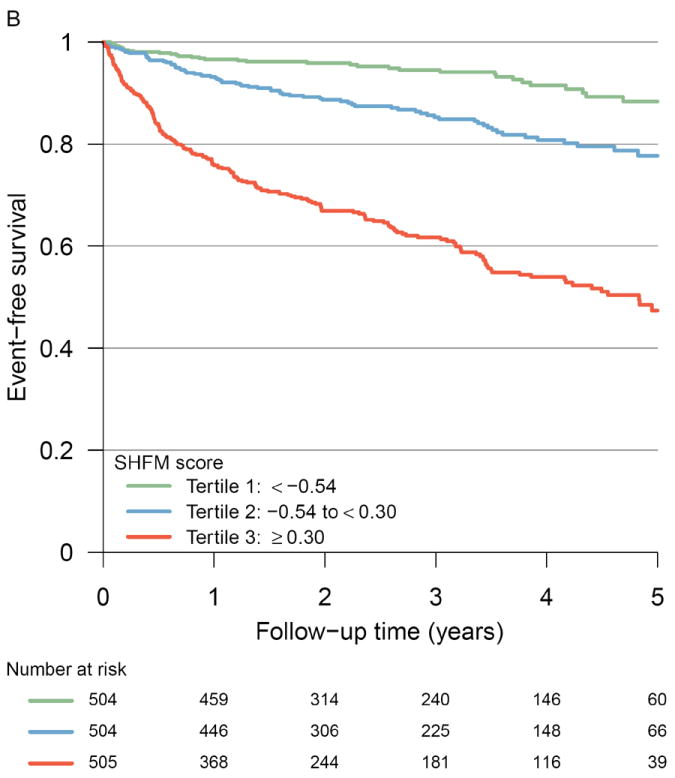
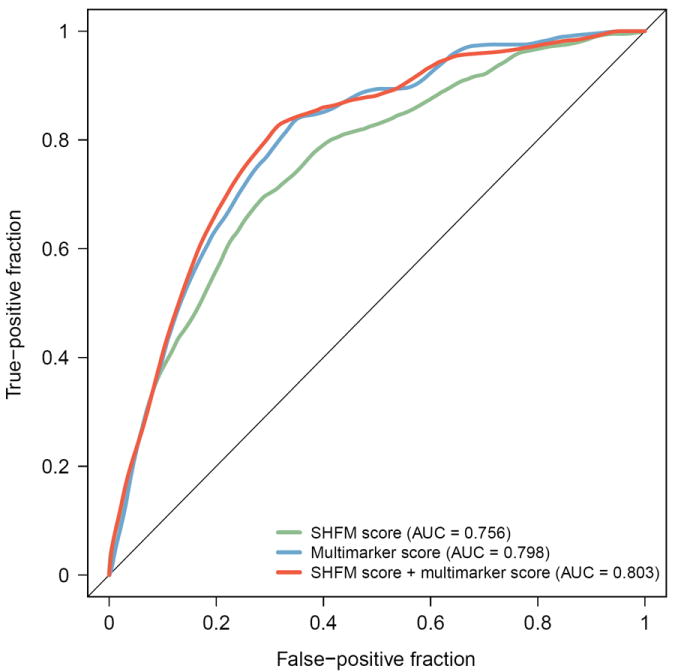
Methods and results: In a multicenter cohort of 1513 chronic systolic heart failure patients, we measured a contemporary biomarker panel consisting of high-sensitivity C-reactive protein, myeloperoxidase, B-type natriuretic peptide, soluble fms-like tyrosine kinase receptor-1, troponin I, soluble toll-like receptor-2, creatinine, and uric acid. From this panel, we calculated a parsimonious multimarker score and assessed its performance in predicting risk of death, cardiac transplantation, or ventricular assist device placement in comparison to an established clinical risk score, the Seattle Heart Failure Model (SHFM). During a median follow-up of 2.5 years, there were 317 outcomes: 187 patients died; 99 were transplanted; and 31 had a ventricular assist device placed. In unadjusted Cox models, patients in the highest tertile of the multimarker score had a 13.7-fold increased risk of adverse outcomes compared with the lowest tertile (95% confidence interval, 8.75-21.5). These effects were independent of the SHFM (adjusted hazard ratio, 6.80; 95% confidence interval, 4.18-11.1). Addition of the multimarker score to the SHFM led to a significantly improved area under the receiver operating characteristic curve of 0.803 versus 0.756 (P=0.003) and appropriately reclassified a significant number of patients who had the outcome into a higher risk category (net reclassification improvement, 25.2%; 95% confidence interval, 14.2-36.2%; P<0.001).
Conclusions: In ambulatory chronic heart failure patients, a score derived from multiple biomarkers integrating diverse biological pathways substantially improves prediction of adverse events beyond current metrics.
Figures
References
-
- Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB, Flegal K, Ford E, Furie K, Go A, Greenlund K, Haase N, Hailpern S, Ho M, Howard V, Kissela B, Kittner S, Lackland D, Lisabeth L, Marelli A, McDermott M, Meigs J, Mozaffarian D, Nichol G, O’Donnell C, Roger V, Rosamond W, Sacco R, Sorlie P, Stafford R, Steinberger J, Thom T, Wasserthiel-Smoller S, Wong N, Wylie-Rosett J, Hong Y. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics--2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119:480–486. - PubMed
-
- Jessup M, Abraham WT, Casey DE, Feldman AM, Francis GS, Ganiats TG, Konstam MA, Mancini DM, Rahko PS, Silver MA, Stevenson LW, Yancy CW. 2009 focused update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009;119:1977–2016. - PubMed
-
- Braunwald E. Biomarkers in heart failure. N Engl J Med. 2008;358:2148–2159. - PubMed
-
- Richards AM. What we may expect from biomarkers in heart failure. Heart Fail Clin. 2009;5:463–470. - PubMed
-
- Cappola TP, Matkovich SJ, Wang W, van Booven D, Li M, Wang X, Qu L, Sweitzer NK, Fang JC, Reilly MP, Hakonarson H, Nerbonne JM, Dorn GW., 2nd Loss-of-function DNA sequence variant in the CLCNKA chloride channel implicates the cardio-renal axis in interindividual heart failure risk variation. Proc Natl Acad Sci U S A. 2011;108:2456–2461. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
