

Interleukin-1β is crucial for the induction of coronary artery inflammation in a mouse model of Kawasaki disease
- PMID: 22361326
- PMCID: PMC3337219
- DOI: 10.1161/CIRCULATIONAHA.111.072769
Interleukin-1β is crucial for the induction of coronary artery inflammation in a mouse model of Kawasaki disease
Abstract
Background: Kawasaki disease (KD) is the most common cause of acute vasculitis and acquired cardiac disease in US children. Untreated, children may develop coronary artery aneurysms, myocardial infarction, and sudden death as a result of the illness. Up to a third of KD patients fail to respond to intravenous immunoglobulin, the standard therapy, and alternative treatments are being investigated. Genetic studies have indicated a possible role for interleukin (IL)-1β in KD. We therefore explored the role of IL-1β in a murine model of KD.
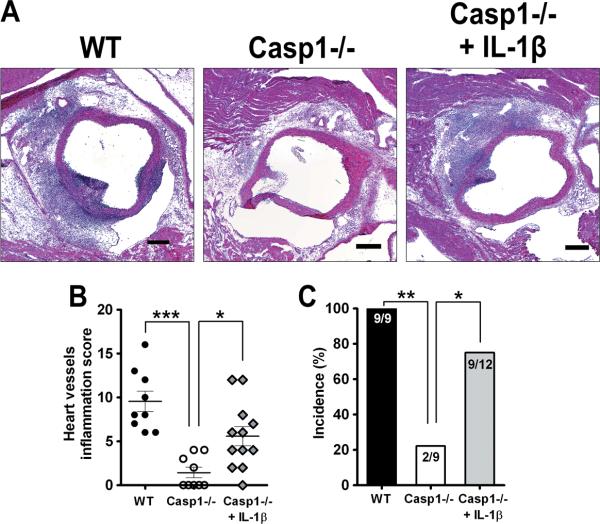
Methods and results: Using an established mouse model of KD that involves injection of Lactobacillus casei cell wall extract (LCWE), we investigated the role of IL-1β and caspase-1 (activated by the inflammasome and required for IL-1β maturation) in coronary arteritis and evaluated the efficacy of IL-1 receptor antagonist as a potential treatment. LCWE-induced IL-1β maturation and secretion were dependent on the NLRP3 inflammasome in macrophages. Both caspase-1-deficient and IL-1 receptor-deficient mice were protected from LCWE-induced coronary lesions. Injection of recombinant IL-1β into caspase-1-deficient mice restored the ability of LCWE to cause coronary lesions in response to LCWE. Furthermore, daily injections of the IL-1 receptor antagonist prevented LCWE-mediated coronary lesions up to 3 days after LCWE injection.
Conclusions: Our results strongly suggest that caspase-1 and IL-1β play critical roles in the development of coronary lesions in this KD mouse model, blocked by IL-1 receptor antagonist. Therefore, anti-IL-1β treatment strategies may constitute an effective, more targeted treatment of KD to prevent coronary lesions.
Figures






Comment in
-
Of mice and children: lessons from a Kawasaki mouse model.Circulation. 2012 Mar 27;125(12):1480-1. doi: 10.1161/CIRCULATIONAHA.112.093930. Epub 2012 Feb 23. Circulation. 2012. PMID: 22361327 No abstract available.
References
-
- Kawasaki T, Kosaki F, Okawa S, Shigematsu I, Yanagawa H. A new infantile acute febrile mucocutaneous lymph node syndrome (mlns) prevailing in japan. Pediatrics. 1974;54:271–276. - PubMed
-
- Burns JC. Kawasaki disease update. Indian J Pediatr. 2009;76:71–76. - PubMed
-
- Newburger JW, Takahashi M, Gerber MA, Gewitz MH, Tani LY, Burns JC, Shulman ST, Bolger AF, Ferrieri P, Baltimore RS, Wilson WR, Baddour LM, Levison ME, Pallasch TJ, Falace DA, Taubert KA, Committee on Rheumatic Fever EdaKD. Young CoCDit. Association AH. Pediatrics AAo Diagnosis, treatment, and long-term management of kawasaki disease: A statement for health professionals from the committee on rheumatic fever, endocarditis and kawasaki disease, council on cardiovascular disease in the young, american heart association. Circulation. 2004;110:2747–2771. - PubMed
-
- Burns JC, Glodé MP. Kawasaki syndrome. Lancet. 2004;364:533–544. - PubMed
-
- Kato H, Sugimura T, Akagi T, Sato N, Hashino K, Maeno Y, Kazue T, Eto G, Yamakawa R. Long-term consequences of kawasaki disease. A 10- to 21-year follow-up study of 594 patients. Circulation. 1996;94:1379–1385. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
