

Prognostic value of a cell cycle progression signature for prostate cancer death in a conservatively managed needle biopsy cohort
- PMID: 22361632
- PMCID: PMC3304411
- DOI: 10.1038/bjc.2012.39
Prognostic value of a cell cycle progression signature for prostate cancer death in a conservatively managed needle biopsy cohort
Abstract
Background: The natural history of prostate cancer is highly variable and it is difficult to predict. We showed previously that a cell cycle progression (CCP) score was a robust predictor of outcome in a conservatively managed cohort diagnosed by transurethral resection of the prostate. A greater need is to predict outcome in patients diagnosed by needle biopsy.
Methods: Total RNA was extracted from paraffin specimens. A CCP score was calculated from expression levels of 31 genes. Clinical variables consisted of centrally re-reviewed Gleason score, baseline prostate-specific antigen level, age, clinical stage, and extent of disease. The primary endpoint was death from prostate cancer.
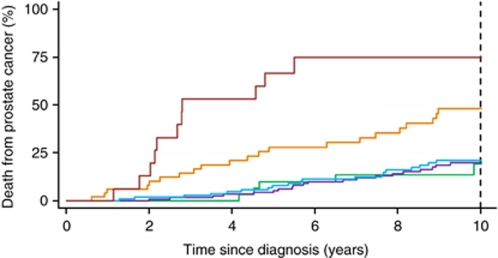
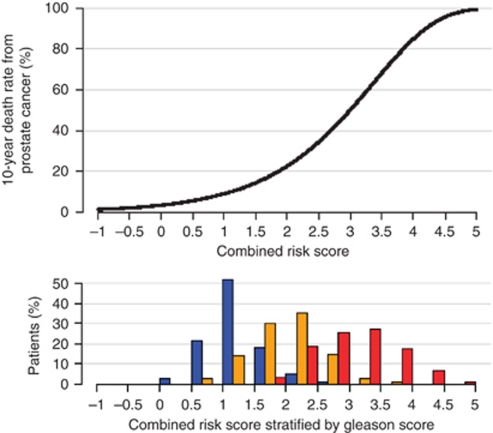
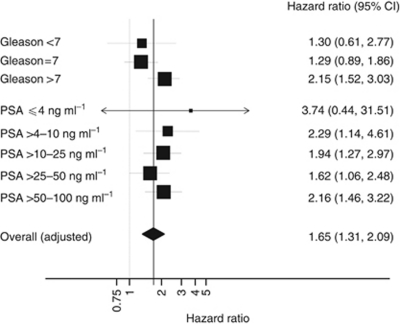
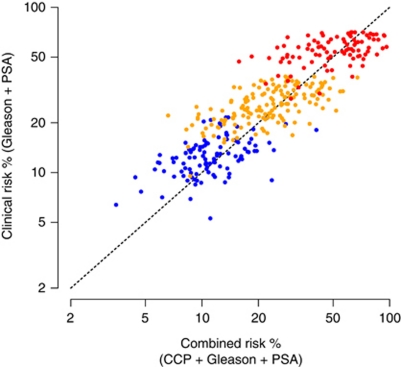
Results: In univariate analysis (n=349), the hazard ratio (HR) for death from prostate cancer was 2.02 (95% CI (1.62, 2.53), P<10(-9)) for a one-unit increase in CCP score. The CCP score was only weakly correlated with standard prognostic factors and in a multivariate analysis, CCP score dominated (HR for one-unit increase=1.65, 95% CI (1.31, 2.09), P=3 × 10(-5)), with Gleason score (P=5 × 10(-4)) and prostate-specific antigen (PSA) (P=0.017) providing significant additional contributions.
Conclusion: For conservatively managed patients, the CCP score is the strongest independent predictor of cancer death outcome yet described and may prove valuable in managing clinically localised prostate cancer.
Conflict of interest statement
Drs Lanchbury, Gutin, Stone, Mr Perry, Mr Park, Mr Younus and Ms Reid are employees of Myriad Genetics. The other authors declare no conflict of interest.
The cell cycle expression profiles were assayed blind to all other data by Myriad Genetics. Analysis was conducted at QMUL under the direction of Professor Cuzick, following a predefined Statistical Analysis Plan. Interpretation of the data was done jointly by all authors, but the final content of this report was determined by non-corporate authors.
Figures
References
-
- Billis A (1986) Latent carcinoma and atypical lesions of prostate. An autopsy study. Urology 4: 324–329 - PubMed
-
- Brawley OW (1997) Prostate carcinoma incidence and patient mortality: the effects of screening and early detection. Cancer 80(9): 1857–1863 - PubMed
-
- Breslow N, Chan CW, Dhom G, Drury RA, Franks LM, Gellei B, Lee YS, Lundberg S, Sparke B, Sternby NH, Tulinius H (1977) Latent carcinoma of prostate at autopsy in seven areas. The International Agency for Research on Cancer, Lyons, France. Int J Cancer 20(5): 680–688 - PubMed
-
- Chou R, Croswell JM, Dana T, Bougatsos C, Blazina I, Fu R, Gleitsmann K, Koenig HC, Lam C, Maltz A, Rugge JB, Lin K (2011) Screening for prostate cancer: a review of the evidence for the US Preventive services task force. Ann Intern Med 155(11): 762–771 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
