

The role of MRI in spinal stab wounds compared with intraoperative findings
- PMID: 22361959
- PMCID: PMC3369065
- DOI: 10.1007/s00586-012-2182-6
The role of MRI in spinal stab wounds compared with intraoperative findings
Abstract
Introduction: Spinal stab wound injuries are quite rare and only few patients have been reported on the basis of MRI scan.
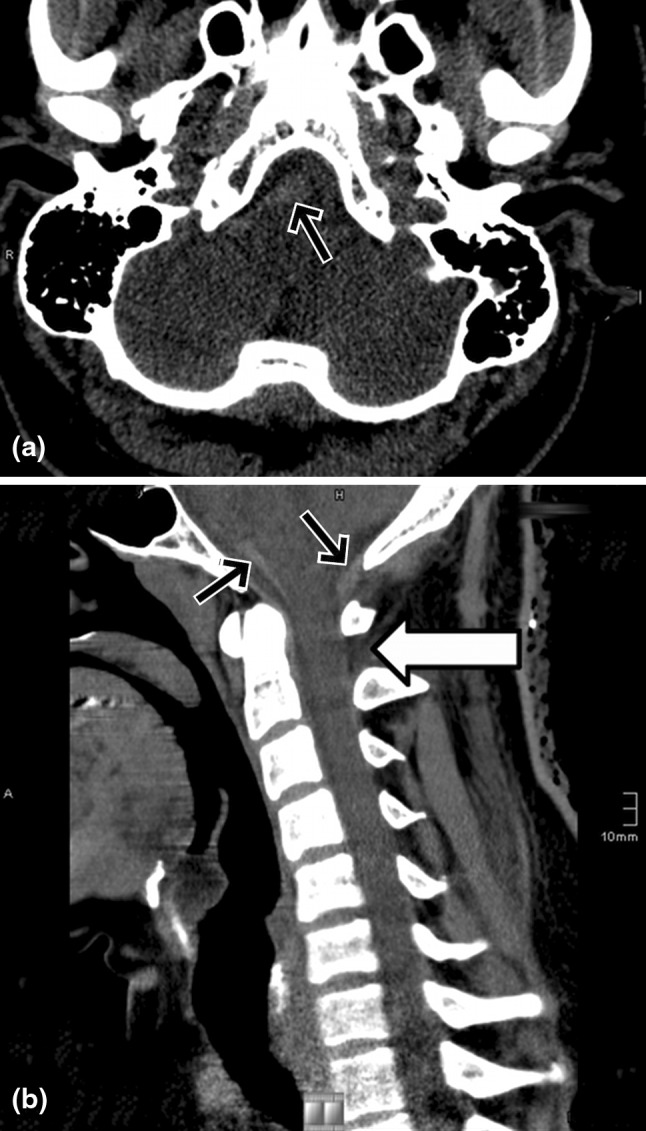
Methods: A 25-year-old man was stabbed at C1/2 and had an incomplete Brown-Sequard syndrome. He underwent surgical exploration because of CSF leakage on the fourth day.
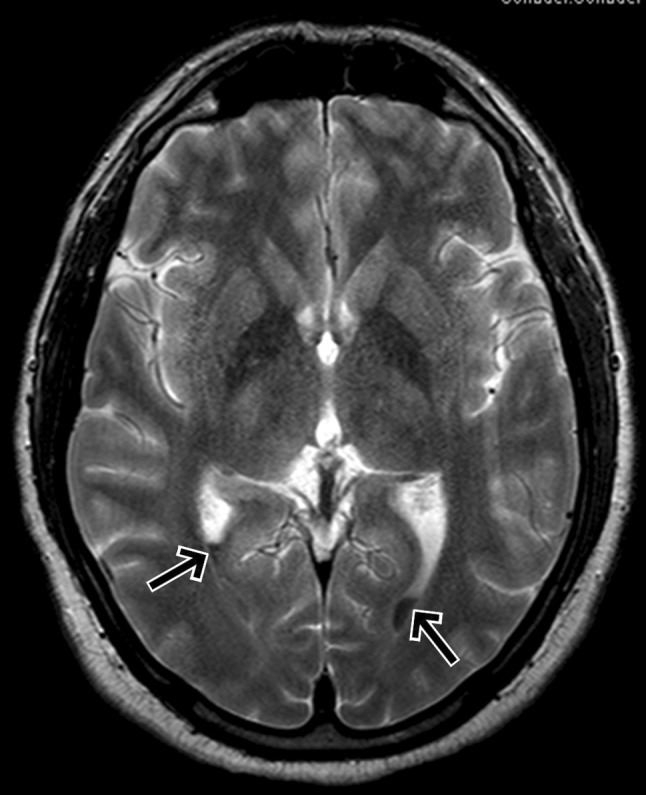
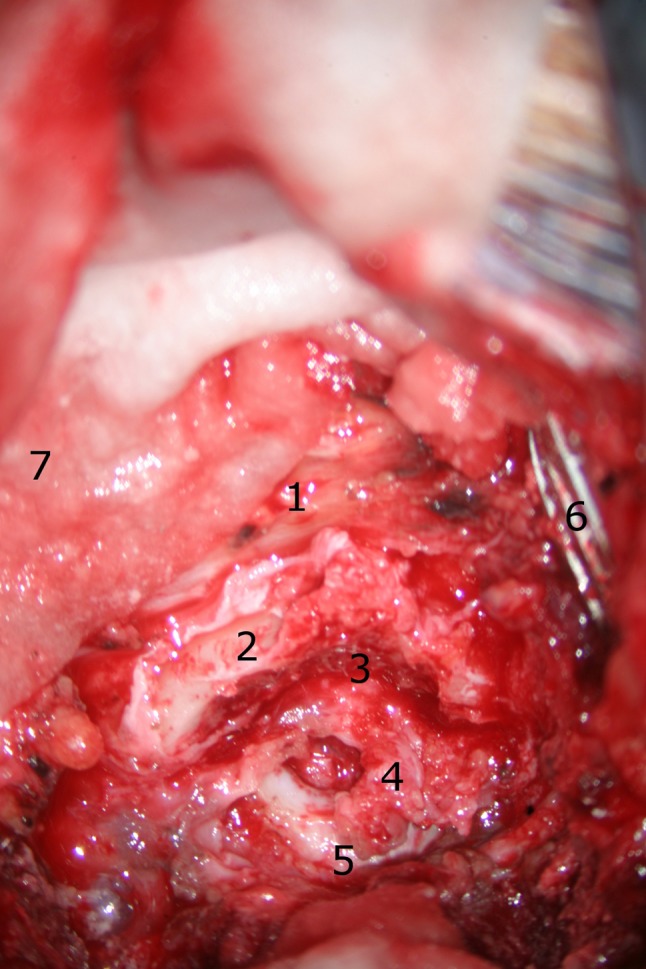
Results: After a follow-up period of 32 months, he was left with a remaining loss of the proprioception of the right foot. We show detailed CT and MR images with the focus on the lesions of the dura and myelon and compared them with intraoperative images. In addition, we contrast our findings with a review of literature published over the last three decades.
Conclusion: MRI gives the most detailed view of soft tissue lesions in SSWs and is in accordance with our intraoperative findings.
Figures







References
-
- Peacock WJ, Shrosbree RD, Key AD. A review of 450 stabwounds of the spinal cord. S Afr Med J. 1977;51:961–964. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
