

Post-operative guidelines following hip arthroscopy
- PMID: 22361976
- PMCID: PMC3535124
- DOI: 10.1007/s12178-011-9107-6
Post-operative guidelines following hip arthroscopy
Abstract
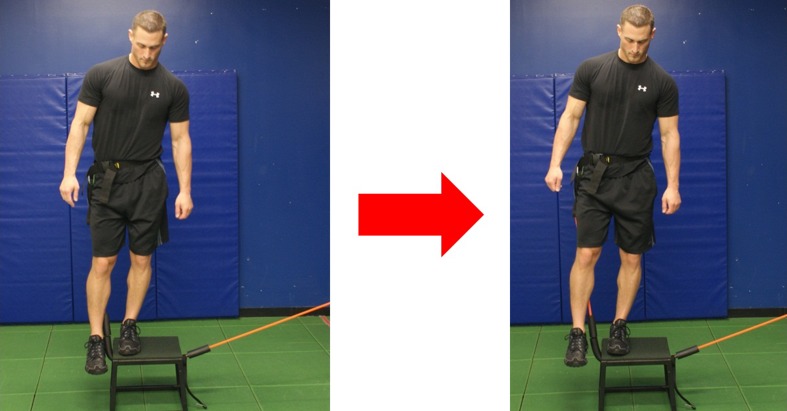
Rehabilitation following hip arthroscopy can vary significantly. Existing programs have been developed as a collaborative effort between physicians and rehabilitation specialists. The evolution of protocol advancement has relied upon feedback from patients, therapists and observable outcomes. Although reports of the first femoroacetabular impingement (FAI) surgeries were reported in the 1930's, it was not until recently that more structured, physiologically based guidelines have been developed and executed. Four phases have been developed in this guideline based on functional and healing milestones achieved which allow the patient to progress to the next level of activity. The goal of Phase I, the protective phase, is to progressively regain 75% of full range of motion (ROM) and normalize gait while respecting the healing process. The primary goal of Phase II is for the patient to gain function and independence in daily activities without discomfort. Rehabilitation goals include uncompensated step up/down on an 8 inch box, as well as, adequate pelvic control during low demand exercises. Phase III goals strive to accomplish pain free, non-compensated recreational activities and higher demand work functions. Manual muscle testing (MMT) grading of 5/5 should be achieved for all hip girdle musculature and an ability to dynamically control body weight in space. Phase IV requires the patient be independent with home and gym programs and be asymptomatic and pain free following workouts. Return to running may be commenced at the 12 week mark, but the proceeding requirements must be achieved. Athletes undergoing the procedure may have an accelerated timetable, based on the underlying pathology. Recognizing the patient's pre-operative health status and post-operative physical demands will direct both the program design and the program timetable.
Figures


References
-
- Ganz R, Parvizi J, Beck M, et al. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003;417:112–120. - PubMed
LinkOut - more resources
Full Text Sources
