

Practical consensus guidelines for the management of enuresis
- PMID: 22362256
- PMCID: PMC3357467
- DOI: 10.1007/s00431-012-1687-7
Practical consensus guidelines for the management of enuresis
Erratum in
- Eur J Pediatr. 2012 Jun;171(6):1005
- Eur J Pediatr. 2013 Feb;172(2):285
Abstract
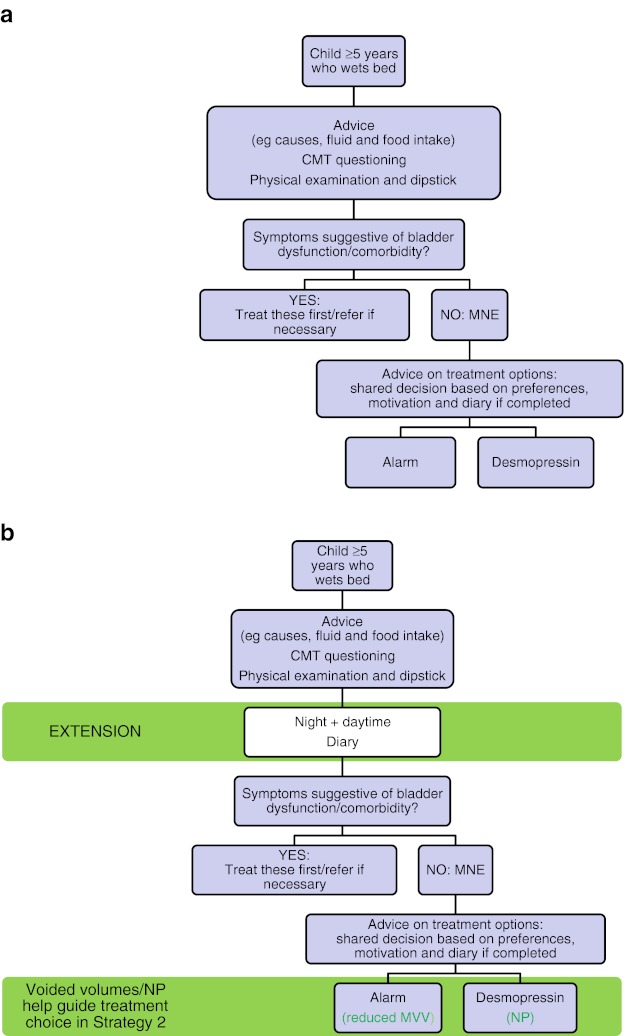
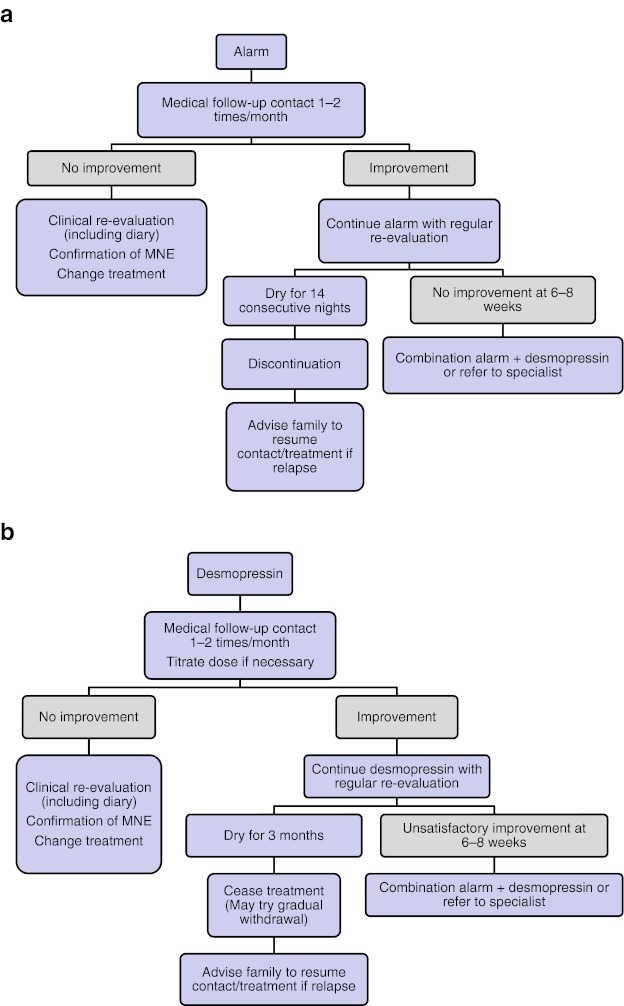
Despite the high prevalence of enuresis, the professional training of doctors in the evaluation and management of this condition is often minimal and/or inconsistent. Therefore, patient care is neither optimal nor efficient, which can have a profound impact on affected children and their families. Once comprehensive history taking and evaluation has eliminated daytime symptoms or comorbidities, monosymptomatic enuresis can be managed efficaciously in the majority of patients. Non-monosymptomatic enuresis is often a more complex condition; these patients may benefit from referral to specialty care centers. We outline two alternative strategies to determine the most appropriate course of care. The first is a basic assessment covering only the essential components of diagnostic investigation which can be carried out in one office visit. The second strategy includes several additional evaluations including completion of a voiding diary, which requires extra time during the initial consultation and two office visits before treatment or specialty referral is provided. This should yield greater success than first-line treatment.
Conclusion: This guideline, endorsed by major international pediatric urology and nephrology societies, aims to equip a general pediatric practice in both primary and secondary care with simple yet comprehensive guidelines and practical tools (i.e., checklists, diary templates, and quick-reference flowcharts) for complete evaluation and successful treatment of enuresis.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
