

Declining in-hospital mortality in patients undergoing coronary bypass surgery in the United States irrespective of presence of type 2 diabetes or congestive heart failure
- PMID: 22362298
- PMCID: PMC6652732
- DOI: 10.1002/clc.21970
Declining in-hospital mortality in patients undergoing coronary bypass surgery in the United States irrespective of presence of type 2 diabetes or congestive heart failure
Abstract
Background: Significant advances in surgical techniques and postsurgical care have been made in the last 10 years. The goal of this study was to evaluate any decline in the age-adjusted in-hospital mortality rate of patients undergoing coronary artery bypass grafting (CABG) using a national database from 1989 to 2004 in the United States.
Hypothesis: Reduction in CABG related mortality in recent years.
Methods: Using the Nationwide Inpatient Sample (NIS) database, we obtained specific ICD-9-CM codes forCABG to compile the data. To exclude nonatherosclerotic cause of coronary disease, we studied only patients older than 40 years. We calculated total and age-adjusted mortality rate per 100,000 for this period.
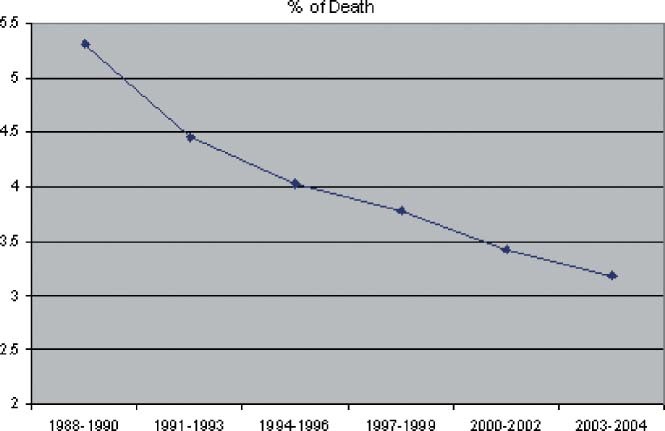
Results: The NIS database contained 1 145 285 patients who had CABG performed from 1988 to 2004. The mean age for these patients was 71.05 ± 9.20 years. From 1989, the age-adjusted rate for all CABG-related mortality has been decreasing steadily and reached the lowest level in 2004: 300.3 per 100 000 in 1989, (95%confidence interval [CI], 20.4-575.9) and 104.69 per 100 000 (95% CI, 22.6-186.7) in 2004. Total death also declined from 5.5% to 3.06%. This decline occurred irrespective of comorbidities such as congestive heart failure, diabetes, or acute myocardial infarction, albeit increasing the number of CABG procedures performed in high-risk patients.
Conclusions: The age-adjusted in-hospital mortality rate from CABG has been declining steadily and reached its lowest level in 2004, irrespective of comorbidities. This decline most likely reflects advances in surgical techniques and the use of evidence-based medicine in patients undergoing CABG.
Figures



Comment in
-
Declining coronary artery bypass-related mortality: more than meets the eye?Clin Cardiol. 2012 May;35(5):261-2. doi: 10.1002/clc.21990. Epub 2012 Apr 23. Clin Cardiol. 2012. PMID: 22528147 Free PMC article.
Similar articles
-
Outcomes in patients undergoing coronary artery bypass graft surgery in the United States based on hospital volume, 2007 to 2011.J Thorac Cardiovasc Surg. 2016 Jun;151(6):1686-92. doi: 10.1016/j.jtcvs.2016.01.050. Epub 2016 Feb 17. J Thorac Cardiovasc Surg. 2016. PMID: 26964912
-
Outcomes and predictors of mortality and stroke after on-pump and off-pump coronary artery bypass surgery in octogenarians.Innovations (Phila). 2013 Jul-Aug;8(4):269-75. doi: 10.1097/IMI.0000000000000000. Innovations (Phila). 2013. PMID: 24145971
-
Comparison of Trends and In-Hospital Outcomes of Concurrent Carotid Artery Revascularization and Coronary Artery Bypass Graft Surgery: The United States Experience 2004 to 2012.JACC Cardiovasc Interv. 2017 Feb 13;10(3):286-298. doi: 10.1016/j.jcin.2016.11.032. JACC Cardiovasc Interv. 2017. PMID: 28183469
-
Prior Percutaneous Coronary Intervention and Mortality in Patients Undergoing Surgical Myocardial Revascularization: Results From the E-CABG (European Multicenter Study on Coronary Artery Bypass Grafting) With a Systematic Review and Meta-Analysis.Circ Cardiovasc Interv. 2018 Feb;11(2):e005650. doi: 10.1161/CIRCINTERVENTIONS.117.005650. Circ Cardiovasc Interv. 2018. PMID: 29440275
-
Percutaneous coronary intervention or coronary artery bypass surgery for cardiogenic shock and multivessel coronary artery disease?Am Heart J. 2010 Jan;159(1):141-7. doi: 10.1016/j.ahj.2009.10.035. Am Heart J. 2010. PMID: 20102880 Review.
Cited by
-
Declining coronary artery bypass-related mortality: more than meets the eye?Clin Cardiol. 2012 May;35(5):261-2. doi: 10.1002/clc.21990. Epub 2012 Apr 23. Clin Cardiol. 2012. PMID: 22528147 Free PMC article.
-
Higher Institutional Volume Reduces Mortality in Reoperative Proximal Thoracic Aortic Surgery.Aorta (Stamford). 2020 Jun;8(3):59-65. doi: 10.1055/s-0040-1713860. Epub 2020 Nov 5. Aorta (Stamford). 2020. PMID: 33152786 Free PMC article.
-
Medanta insulin protocols in patients undergoing cardiac surgery.Indian J Endocrinol Metab. 2014 Jul;18(4):455-67. doi: 10.4103/2230-8210.137486. Indian J Endocrinol Metab. 2014. PMID: 25143899 Free PMC article. Review.
-
Perioperative outcomes of coronary artery bypass graft surgery in Johannesburg, South Africa.J Cardiothorac Surg. 2021 Jan 7;16(1):7. doi: 10.1186/s13019-020-01385-8. J Cardiothorac Surg. 2021. PMID: 33413554 Free PMC article.
-
Impact of early quantitative morbidity on 1-year outcomes in coronary artery bypass graft surgery.Interact Cardiovasc Thorac Surg. 2022 Mar 31;34(4):523-531. doi: 10.1093/icvts/ivab316. Interact Cardiovasc Thorac Surg. 2022. PMID: 34788466 Free PMC article. Clinical Trial.
References
-
- Lloyd‐Jones D, Adams R, Carnethon M, et al. Heart disease and stroke statistics–2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119:480–486. - PubMed
-
- Coronary artery surgery study (CASS): a randomized trial of coronary artery bypass surgery. Quality of life in patients randomly assigned to treatment groups. Circulation. 1983;68:951–960. - PubMed
-
- Coronary artery surgery study (CASS): a randomized trial of coronary artery bypass surgery. Survival data. Circulation. 1983;68:939–950. - PubMed
-
- Alderman EL, Fisher LD, Litwin P, et al. Results of coronary artery surgery in patients with poor left ventricular function (CASS). Circulation. 1983;68:785–795. - PubMed
-
- Tarantini G, Ramondo A, Napodano M, et al. PCI versus CABG for multivessel coronary disease in diabetics. Catheter Cardiovasc Interv. 2009;73:50–58. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
