An inflamed trichilemmal (pilar) cyst: Not so simple?
- PMID: 22362454
- PMCID: PMC3271400
- DOI: 10.4297/najms.2011.3431
An inflamed trichilemmal (pilar) cyst: Not so simple?
Abstract
Context: Trichilemmal (pilar) cysts are common skin lesions that often present on the scalps of mature men and women. These cysts often become inflamed when the wall of the cyst ruptures, but few reports have addressed the immunologic features of this process.
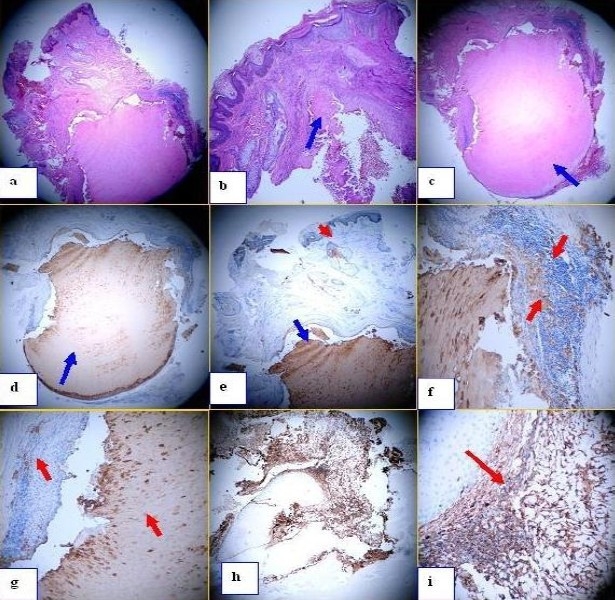
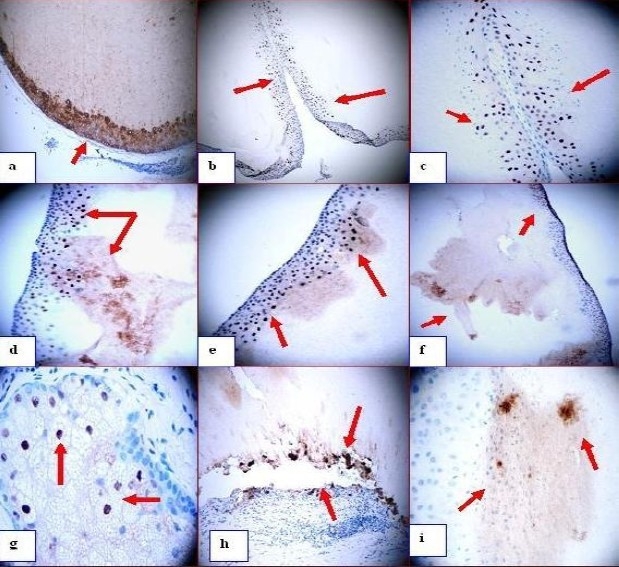
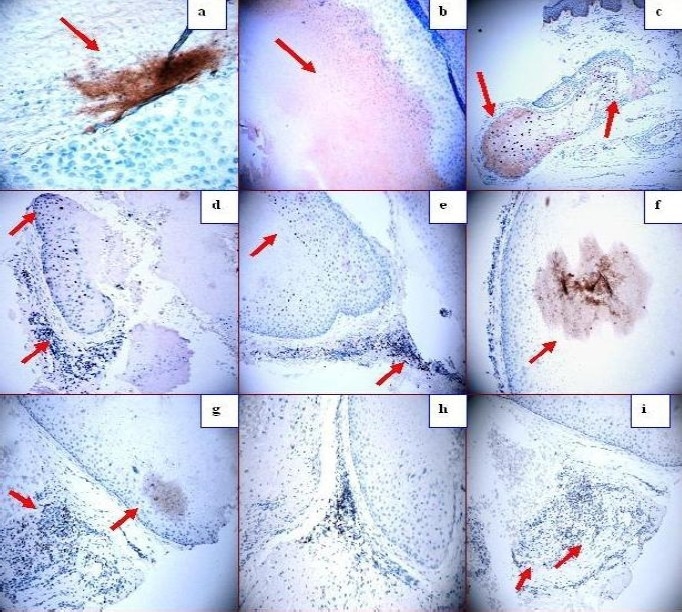
Case report: A 22-year-old female presented with rapidly growing nodule on her left cheek, with evidence of acute inflammation. Skin tissue for hematoxylin and eosin examination, as well as for immunohistochemical analysis was taken and reviewed. As controls, we utilized two archival, non-inflamed trichilemmal cysts. Hematoxylin and eosin staining demonstrated classic features of an inflamed trichilemmal cyst. No cytologic atypia was noted, and no significant number of mitotic figures was identified. Immunohistochemistry stains revealed that several cell cycle/tumor suppressor/apoptotic markers, antigen presenting cell markers, metalloproteinases and T cell response markers were highly expressed inside and around the disrupted cyst. The control, non-inflamed cysts were negative for the same markers. CD1a was also appreciated within the epidermis, suprajacent to the inflamed cyst.
Conclusions: Upregulation and/or downregulation of selected cell cycle regulator and/or tumor suppressor/apoptotic markers, as well as antigen presenting cells and some protein kinases could recruit and activate T lymphocytes and other inflammatory cells to the non-disrupted cyst for unknown reasons. The immune response may be involved in the initial cyst rupture, or induced by an unknown alteration in the cyst. Larger studies are needed to address these questions.
Keywords: BCL-10; Trichilemmal (pilar) cyst; cytokeratin A1/A3; matrix metalloproteinase-9 (MMP9); p27kip1; vimentin.
Figures
Similar articles
-
Morphological spectrum of pilar cysts.N Am J Med Sci. 2013 Feb;5(2):124-8. doi: 10.4103/1947-2714.107532. N Am J Med Sci. 2013. PMID: 23641374 Free PMC article.
-
Cytodiagnosis of simple and proliferating trichilemmal cysts.Acta Cytol. 2001 Jul-Aug;45(4):582-8. doi: 10.1159/000327868. Acta Cytol. 2001. PMID: 11480722
-
In situ carcinoma in a hybrid cyst: a case report.J Cutan Pathol. 2017 Feb;44(2):189-192. doi: 10.1111/cup.12852. Epub 2016 Dec 1. J Cutan Pathol. 2017. PMID: 27792259
-
Follicular hybrid cysts. An expanded spectrum.Am J Dermatopathol. 1991 Jun;13(3):228-33. doi: 10.1097/00000372-199106000-00003. Am J Dermatopathol. 1991. PMID: 1714246 Review.
-
Merkel cell carcinoma in situ arising in a trichilemmal cyst: a case report and literature review.Am J Dermatopathol. 2008 Oct;30(5):458-61. doi: 10.1097/DAD.0b013e31817a9896. Am J Dermatopathol. 2008. PMID: 18806489 Review.
Cited by
-
A rare ossifying trichilemmal cyst in a young female patient: a case report and literature review.Dermatol Reports. 2022 Sep 16;15(2):9569. doi: 10.4081/dr.2022.9569. eCollection 2023 Jun 7. Dermatol Reports. 2022. PMID: 37397402 Free PMC article.
-
Immune reactivity in psoriatic munro-saboureau microabscesses, stratum corneum and blood vessels.N Am J Med Sci. 2012 Jun;4(6):257-65. doi: 10.4103/1947-2714.97204. N Am J Med Sci. 2012. PMID: 22754876 Free PMC article.
-
Scrotal trichilemmal cysts: a case report.Ann Med Surg (Lond). 2023 Apr 14;85(5):2166-2168. doi: 10.1097/MS9.0000000000000666. eCollection 2023 May. Ann Med Surg (Lond). 2023. PMID: 37229016 Free PMC article.
-
A Large Pilar Sheath Acanthoma of the Cheek Successfully Treated With Surgical Excision.Cureus. 2024 Jun 14;16(6):e62364. doi: 10.7759/cureus.62364. eCollection 2024 Jun. Cureus. 2024. PMID: 39006610 Free PMC article.
-
Giant trichilemmal cyst of scrotum.J Cutan Aesthet Surg. 2024 Jul-Sep;17(3):249-251. doi: 10.4103/JCAS.JCAS_43_21. Epub 2022 Dec 2. J Cutan Aesthet Surg. 2024. PMID: 39483648 Free PMC article.
References
-
- Anolik R, Firoz B, Walters RF, et al. Proliferating trichilemmal cyst with focal calcification. Dermatology Online J. 2008;14:25. - PubMed
-
- McKee PH, et al., editors. Pathology of the Skin with Clinical Correlations. 3rd ed. China: Mosby; 2005. Cutaneous cysts; p. 1670.
-
- Abreu Velez AM, Girard JG, Howard MS. IgG bullous pemphigoid with antibodies to IgD, dermal blood vessels, eccrine glands and the endomysium of monkey esophagus. Ms in press. N Dermatol Online. 2011;2:48–51.
-
- Howard MS, Yepes MM, Maldonado-Estrada JG, et al. Broad histopathologic patterns of non-glabrous skin and glabrous skin from patients with a new variant of endemic pemphigus foliaceus-part 1. J Cutan Pathol. 2010;37:222–223. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous