

Salvage Resection for Isolated Local and/or Regional Failure of Head/Neck Cancer Following Definitive Concurrent Chemoradiotherapy Case Series and Review of the Literature
- PMID: 22363192
- PMCID: PMC3277417
Salvage Resection for Isolated Local and/or Regional Failure of Head/Neck Cancer Following Definitive Concurrent Chemoradiotherapy Case Series and Review of the Literature
Abstract
Background: Primary management of advanced head/neck cancers involves concurrent chemoradiotherapy . Subsequently, regional and local failures are managed with resection but there have been few reports that describe the morbidity and disease control outcomes of surgical salvage in this setting.
Methods: Retrospective analysis describes complications, survival, and patterns of failure after salvage resection of isolated local and/or regional failures of head/neck cancer following definitive concurrent chemoradiotherapy.
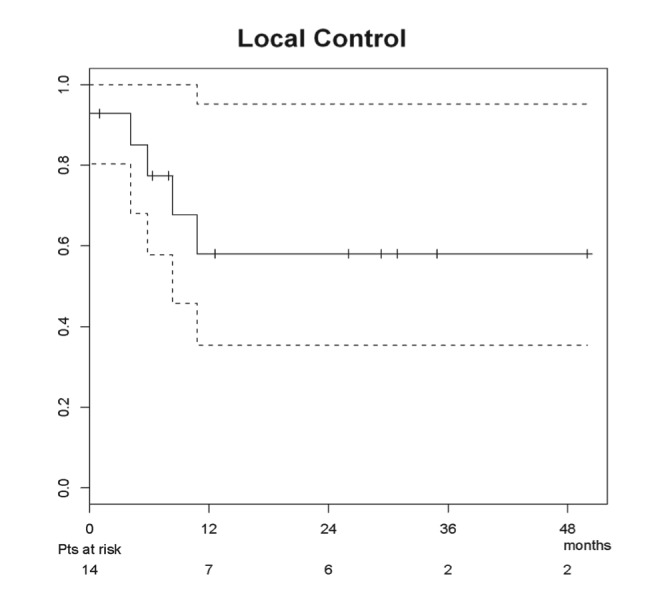
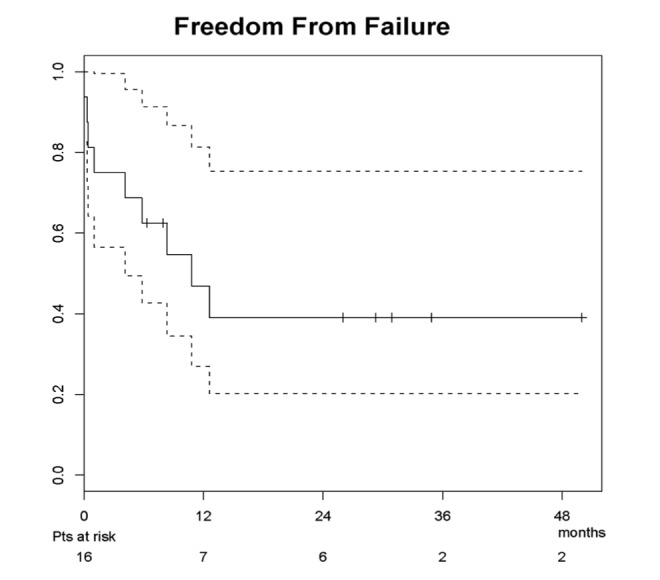
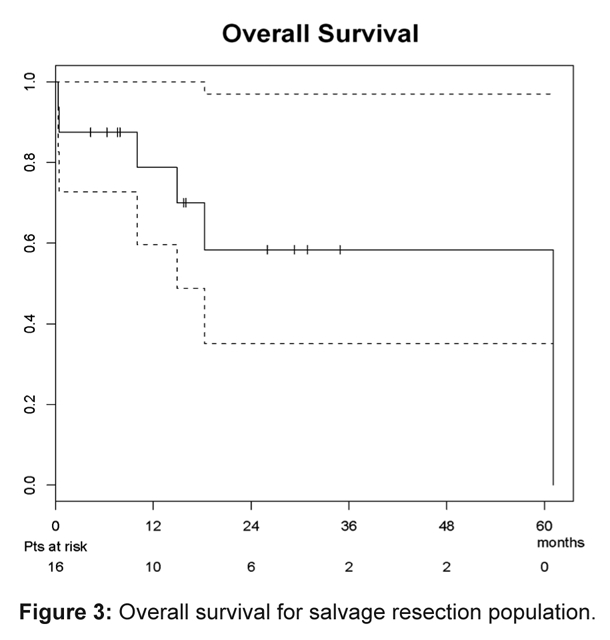
Results: Sixteen patients were identified for inclusion: laryngectomy in 11 patients, oral cavity/oropharynx resection in 2 patients, and neck dissection alone in 4 patients. Ten patients required graft tissue reconstruction (6 pedicle and 4 free flap). Median post-operative hospitalization was 7 days (range 3-19), and 4 patients required hospital re-admission. At a median survivor follow-up of 15.8 months (range 4.3-34.9), 10 patients were alive (6 without evidence of disease). Seven patients experienced disease recurrence at a median 6.7 months (range 0-12.6) following salvage resection (2 with isolated distant failures). Estimated 2-year local/regional control, freedom from failure, and overall survival were 58%, 39%, and 58%, respectively.
Conclusions: Surgical salvage after primary definitive concurrent chemoradiotherapy is feasible with toxicity and outcomes similar to prior radiotherapy alone or sequential chemotherapy and radiation. Local andregional recurrence remains the predominant pattern of failure.
Keywords: Combined modality therapy; Head and neck neoplasms; Organ preservation therapy; Salvage therapy.
Figures
References
-
- Forastiere A, Koch W, Trotti A, Sidransky D. Head and neck cancer. N Engl J Med. 2001;345:1890–1900. - PubMed
-
- Cooper JS, Pajak TF, Forastiere AA, et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med. 2004;350:1937–1944. - PubMed
-
- Bernier J, Domenge C, Ozsahin M, et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med. 2004;350:1945–1952. - PubMed
-
- Goodwin WJ. Salvage surgery for patients with recurrent squamous cell carcinoma of the upper aerodigestive tract: when do the ends justify the means? Laryngoscope. 2000;110(suppl 93):1–18. - PubMed
-
- Forastiere AA, Goepfert H, Maor M, et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med. 2003;349:2091–2098. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources