

Are long-term non-progressors very slow progressors? Insights from the Chelsea and Westminster HIV cohort, 1988-2010
- PMID: 22363409
- PMCID: PMC3282685
- DOI: 10.1371/journal.pone.0029844
Are long-term non-progressors very slow progressors? Insights from the Chelsea and Westminster HIV cohort, 1988-2010
Abstract
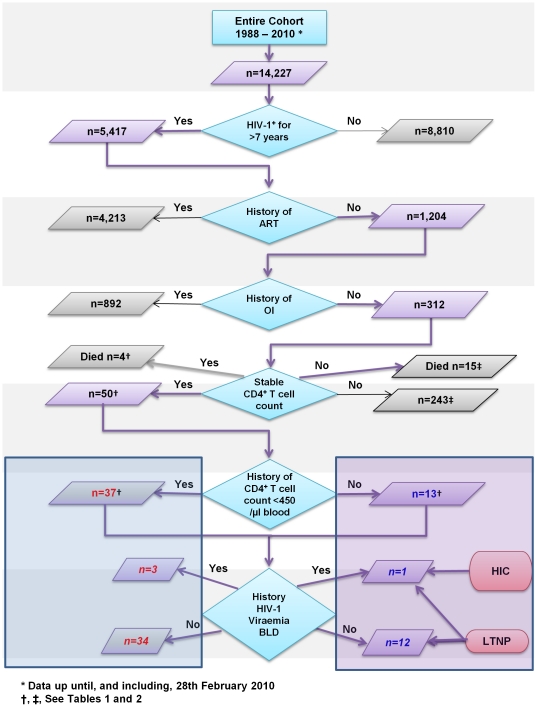
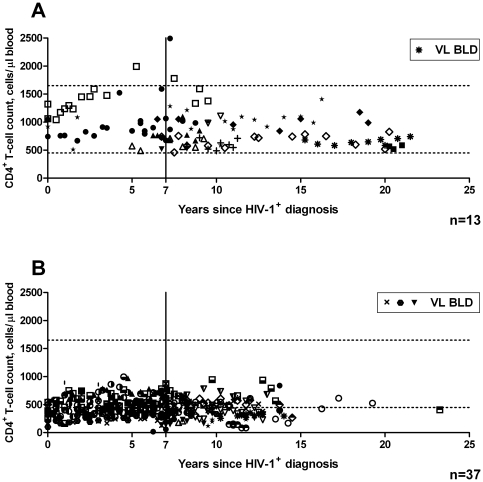
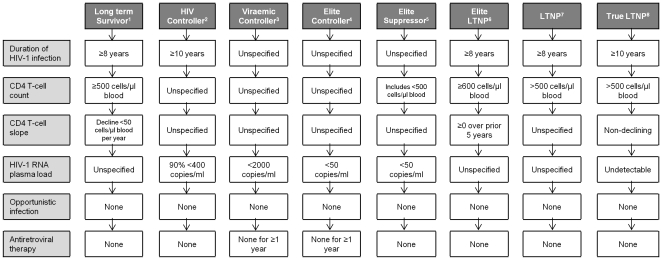
Define and identify long-term non-progressors (LTNP) and HIV controllers (HIC), and estimate time until disease progression. LTNP are HIV-1(+) patients who maintain stable CD4(+) T-cell counts, with no history of opportunistic infection or antiretroviral therapy (ART). HIC are a subset of LTNP who additionally have undetectable viraemia. These individuals may provide insights for prophylactic and therapeutic development. Records of HIV-1(+) individuals attending Chelsea and Westminster Hospital (1988-2010), were analysed. LTNP were defined as: HIV-1(+) for >7 years; ART-naïve; no history of opportunistic infection and normal, stable CD4(+) T-cell counts. MIXED procedure in SAS using random intercept model identified long-term stable CD4(+) T-cell counts. Survival analysis estimated time since diagnosis until disease progression. Subjects exhibiting long-term stable CD4(+) T-cell counts with history below the normal range (<450 cells/µl blood) were compared to LTNP whose CD4(+) T-cell count always remained normal. Within these two groups subjects with HIV-1 RNA load below limit of detection (BLD) were identified. Of 14,227 patients, 1,204 were diagnosed HIV-1(+) over 7 years ago and were ART-naïve. Estimated time until disease progression for the 20% (239) whose CD4(+) T-cell counts remained within the normal range, was 6.2 years (IQR: 2.0 to 9.6); significantly longer than 4.0 years (IQR: 1.0 to 7.3) for patients with historical CD4(+) T-cell count below normal (Logrank chi-squared = 21.26; p<0.001). Within a subpopulation of 312 asymptomatic patients, 50 exhibited long-term stable CD4(+) T-cell counts. Of these, 13 were LTNP, one of whom met HIC criteria. Of the remaining 37 patients with long-term stable low CD4(+) T-cell counts, 3 controlled HIV-1 RNA load BLD. Individuals with stable, normal CD4(+) T-cell counts progressed less rapidly than those with low CD4(+) T-cell counts. Few LTNP and HIC identified in this and other studies, endorse the need for universal definitions to facilitate comparison.
Conflict of interest statement
Figures
Similar articles
-
Differences in disease progression in a cohort of long-term non-progressors after more than 16 years of HIV-1 infection.AIDS. 2004 May 21;18(8):1109-16. doi: 10.1097/00002030-200405210-00004. AIDS. 2004. PMID: 15166526
-
Effect of antiretroviral therapy on the mortality of HIV-1 infection long-term non-progressors: a cohort study.BMC Infect Dis. 2025 Jan 16;25(1):72. doi: 10.1186/s12879-025-10448-x. BMC Infect Dis. 2025. PMID: 39819447 Free PMC article.
-
Mechanisms of HIV non-progression; robust and sustained CD4+ T-cell proliferative responses to p24 antigen correlate with control of viraemia and lack of disease progression after long-term transfusion-acquired HIV-1 infection.Retrovirology. 2008 Dec 11;5:112. doi: 10.1186/1742-4690-5-112. Retrovirology. 2008. PMID: 19077215 Free PMC article.
-
Omic Technologies in HIV: Searching Transcriptional Signatures Involved in Long-Term Non-Progressor and HIV Controller Phenotypes.Front Immunol. 2022 Jul 1;13:926499. doi: 10.3389/fimmu.2022.926499. eCollection 2022. Front Immunol. 2022. PMID: 35844607 Free PMC article. Review.
-
Comparison of the Biological Basis for Non-HIV Transmission to HIV-Exposed Seronegative Individuals, Disease Non-Progression in HIV Long-Term Non-Progressors and Elite Controllers.Viruses. 2023 Jun 13;15(6):1362. doi: 10.3390/v15061362. Viruses. 2023. PMID: 37376660 Free PMC article. Review.
Cited by
-
Increased Prevalence of Unstable HLA-C Variants in HIV-1 Rapid-Progressor Patients.Int J Mol Sci. 2022 Nov 27;23(23):14852. doi: 10.3390/ijms232314852. Int J Mol Sci. 2022. PMID: 36499177 Free PMC article.
-
Loss of long-term non-progressor and HIV controller status over time in the French Hospital Database on HIV - ANRS CO4.PLoS One. 2017 Oct 2;12(10):e0184441. doi: 10.1371/journal.pone.0184441. eCollection 2017. PLoS One. 2017. PMID: 28968404 Free PMC article.
-
Broadly neutralizing antibodies for HIV prevention: a comprehensive review and future perspectives.Clin Microbiol Rev. 2024 Jun 13;37(2):e0015222. doi: 10.1128/cmr.00152-22. Epub 2024 Apr 30. Clin Microbiol Rev. 2024. PMID: 38687039 Free PMC article. Review.
-
Gut Microbiota in HIV Infection: Implication for Disease Progression and Management.Gastroenterol Res Pract. 2014;2014:803185. doi: 10.1155/2014/803185. Epub 2014 Jun 12. Gastroenterol Res Pract. 2014. PMID: 25024700 Free PMC article. Review.
-
Indian Long-term Non-Progressors Show Broad ADCC Responses with Preferential Recognition of V3 Region of Envelope and a Region from Tat Protein.Front Immunol. 2017 Jan 19;8:5. doi: 10.3389/fimmu.2017.00005. eCollection 2017. Front Immunol. 2017. PMID: 28154562 Free PMC article.
References
-
- Clerici M, Stocks NI, Zajac RA, Boswell RN, Lucey DR, et al. Detection of three distinct patterns of T helper cell dysfunction in asymptomatic, human immunodeficiency virus-seropositive patients. Independence of CD4+ cell numbers and clinical staging. J Clin Invest. 1989;84(6):1892–1899. - PMC - PubMed
-
- Imami N, Hardy G, Burton C, Pires A, Pido-Lopez J, et al. Immune responses and reconstitution in HIV-1 infected individuals: impact of anti-retroviral therapy, cytokines and therapeutic vaccination. Immunol Lett. 2001;79(1–2):63–76. - PubMed
-
- Pantaleo G, Fauci AS. Immunopathogenesis of HIV infection. Annu Rev Microbiol. 1996;50:825–854. - PubMed
-
- CDC. From the Centers for Disease Control and Prevention. 1993 revised classification system for HIV infection and expanded surveillance case definition for AIDS among adolescents and adults. JAMA. 1993;269(6):729–730. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
