

Feasibility of modified surviving sepsis campaign guidelines in a resource-restricted setting based on a cohort study of severe S. aureus sepsis [corrected]
- PMID: 22363410
- PMCID: PMC3283614
- DOI: 10.1371/journal.pone.0029858
Feasibility of modified surviving sepsis campaign guidelines in a resource-restricted setting based on a cohort study of severe S. aureus sepsis [corrected]
Erratum in
- PLoS One. 2012;7(5): doi/10.1371/annotation/7f498e31-2709-44f6-877a-d0ee89bebe03
Abstract
Background: The Surviving Sepsis Campaign (SSC) guidelines describe best practice for the management of severe sepsis and septic shock in developed countries, but most deaths from sepsis occur where healthcare is not sufficiently resourced to implement them. Our objective was to define the feasibility and basis for modified guidelines in a resource-restricted setting.
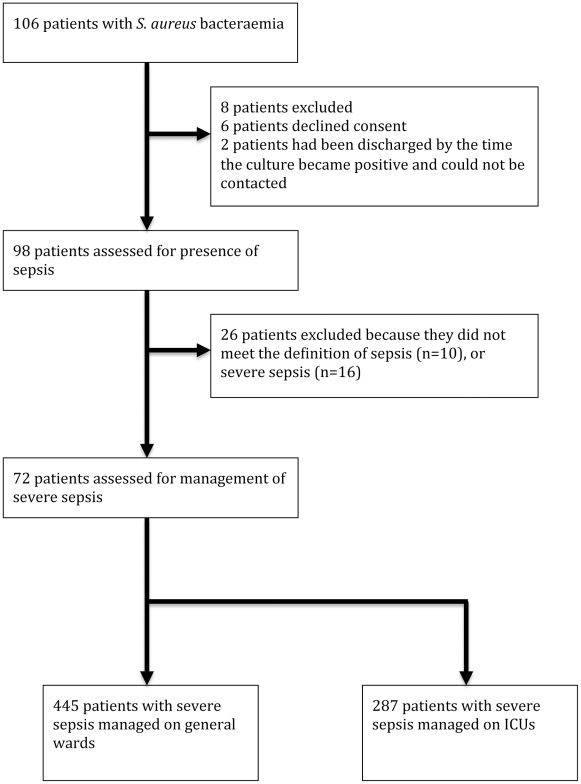
Methods and findings: We undertook a detailed assessment of sepsis management in a prospective cohort of patients with severe sepsis caused by a single pathogen in a 1,100-bed hospital in lower-middle income Thailand. We compared their management with the SSC guidelines to identify care bundles based on existing capabilities or additional activities that could be undertaken at zero or low cost. We identified 72 patients with severe sepsis or septic shock associated with S. aureus bacteraemia, 38 (53%) of who died within 28 days. One third of patients were treated in intensive care units (ICUs). Numerous interventions described by the SSC guidelines fell within existing capabilities, but their implementation was highly variable. Care available to patients on general wards covered the fundamental principles of sepsis management, including non-invasive patient monitoring, antimicrobial administration and intravenous fluid resuscitation. We described two additive care bundles, one for general wards and the second for ICUs, that if consistently performed would be predicted to improve outcome from severe sepsis.
Conclusion: It is feasible to implement modified sepsis guidelines that are scaled to resource availability, and that could save lives prior to the publication of international guidelines for developing countries.
Conflict of interest statement
References
-
- Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. 1992. Chest. 2009;136:e28. - PubMed
-
- Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Intensive Care Med. 2003;29:530–538. - PubMed
-
- World Health Organization. The global burden of disease: 2004 update: Available: http://www.who.int/healthinfo/global_burden_disease/2004_report_update/e.... Accessed 2011 Dec 25.
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348:1546–1554. - PubMed
-
- World Health Organization. The World Health Report 1996 - Fighting disease, fostering development: Available: http://www.who.int/whr/1996/en/index.html. Accessed 2011 Dec 25.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
