

Early and individualized goal-directed therapy for trauma-induced coagulopathy
- PMID: 22364525
- PMCID: PMC3306198
- DOI: 10.1186/1757-7241-20-15
Early and individualized goal-directed therapy for trauma-induced coagulopathy
Abstract
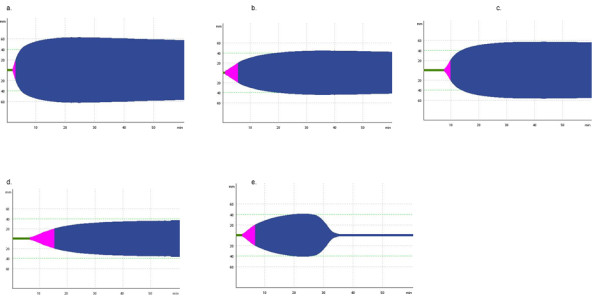
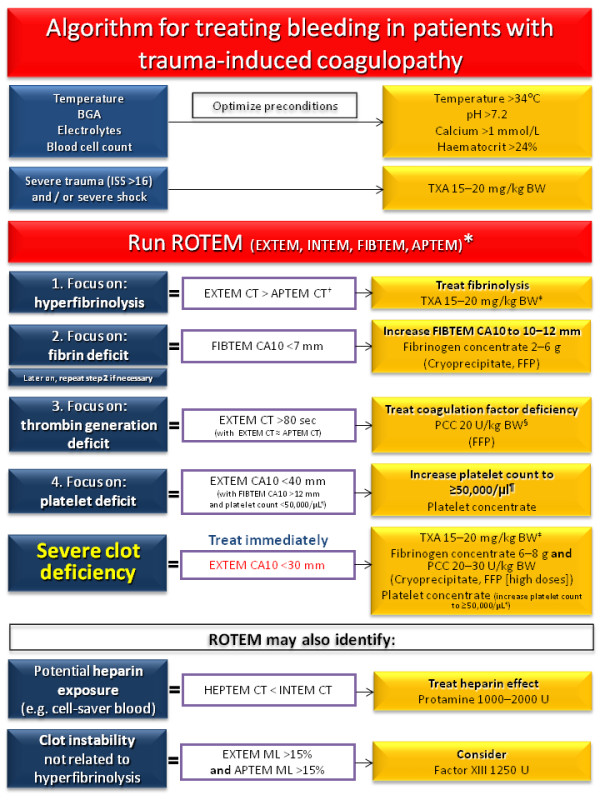
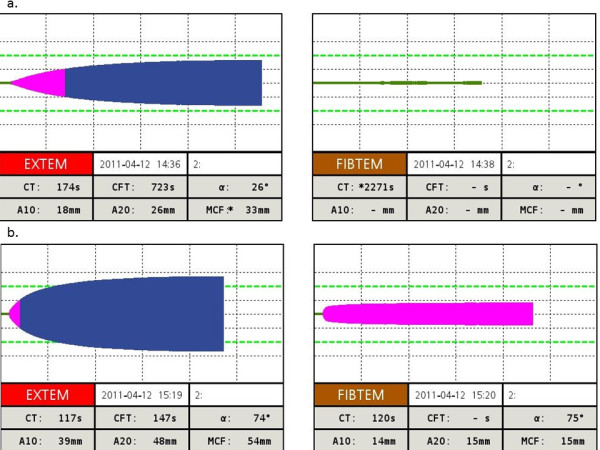
Severe trauma-related bleeding is associated with high mortality. Standard coagulation tests provide limited information on the underlying coagulation disorder. Whole-blood viscoelastic tests such as rotational thromboelastometry or thrombelastography offer a more comprehensive insight into the coagulation process in trauma. The results are available within minutes and they provide information about the initiation of coagulation, the speed of clot formation, and the quality and stability of the clot. Viscoelastic tests have the potential to guide coagulation therapy according to the actual needs of each patient, reducing the risks of over- or under-transfusion. The concept of early, individualized and goal-directed therapy is explored in this review and the AUVA Trauma Hospital algorithm for managing trauma-induced coagulopathy is presented.
Figures
References
-
- Sauaia A, Moore FA, Moore EE, Moser KS, Brennan R, Read RA, Pons PT. Epidemiology of trauma deaths: a reassessment. J Trauma. 1995;38(2):185–193. - PubMed
-
- Tien HC, Spencer F, Tremblay LN, Rizoli SB, Brenneman FD. Preventable deaths from hemorrhage at a level I Canadian trauma center. J Trauma. 2007;62(1):142–146. - PubMed
-
- Brohi K, Singh J, Heron M, Coats T. Acute traumatic coagulopathy. J Trauma. 2003;54(6):1127–1130. - PubMed
-
- Maegele M, Lefering R, Yucel N, Tjardes T, Rixen D, Paffrath T, Simanski C, Neugebauer E, Bouillon B. Early coagulopathy in multiple injury: an analysis from the German Trauma Registry on 8724 patients. Injury. 2007;38(3):298–304. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
