

Screening for chronic cerebrospinal venous insufficiency (CCSVI) using ultrasound: recommendations for a protocol
- PMID: 22364944
- PMCID: PMC3814564
Screening for chronic cerebrospinal venous insufficiency (CCSVI) using ultrasound: recommendations for a protocol
Abstract
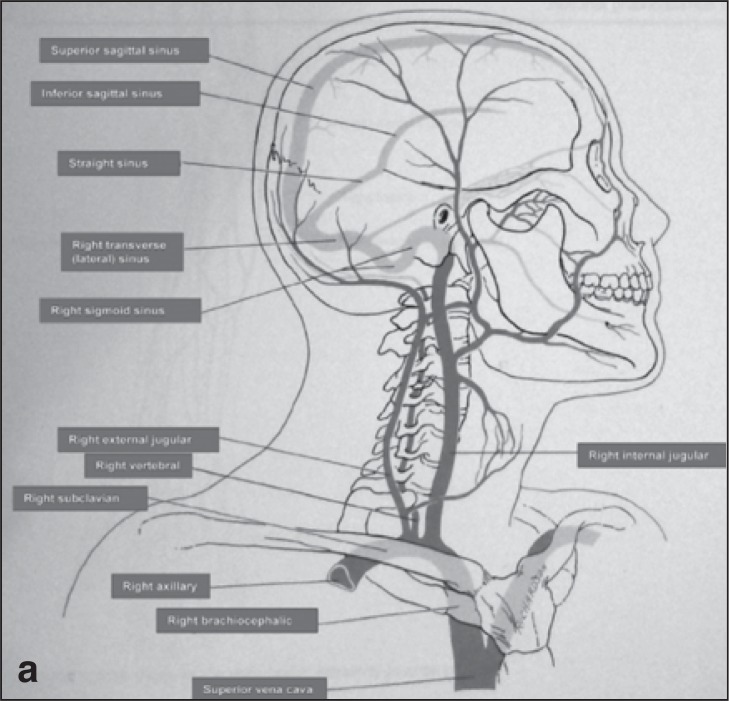
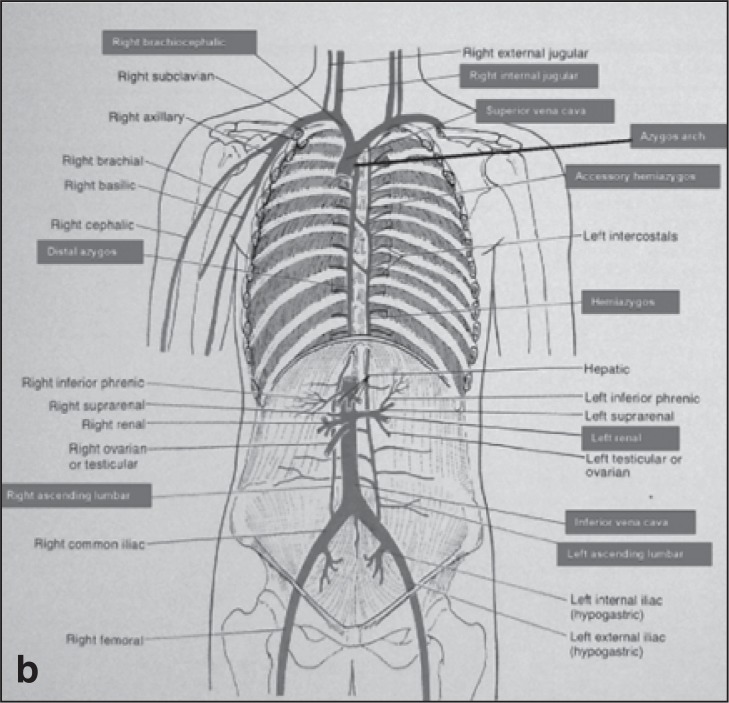
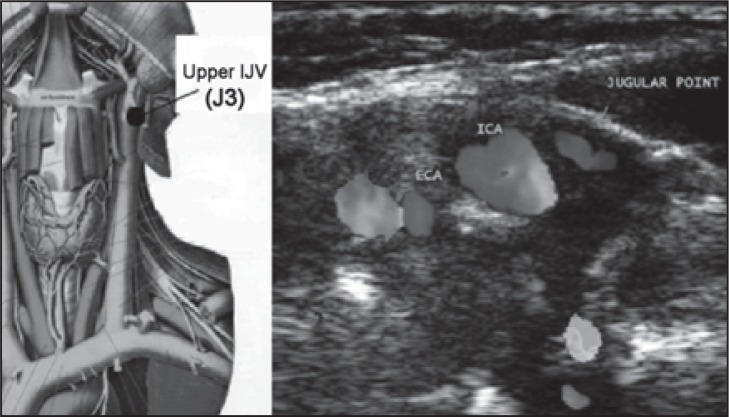
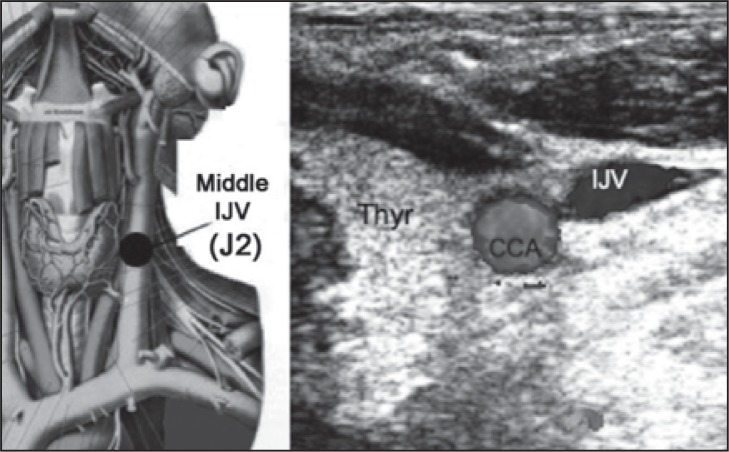
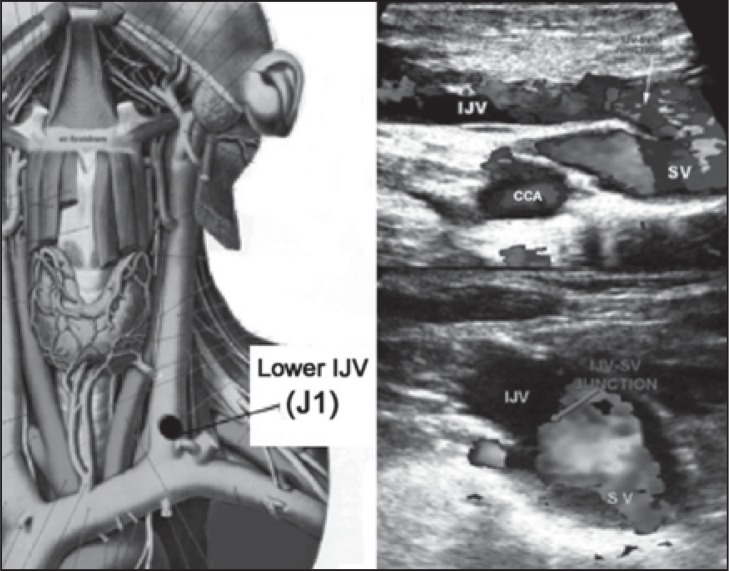
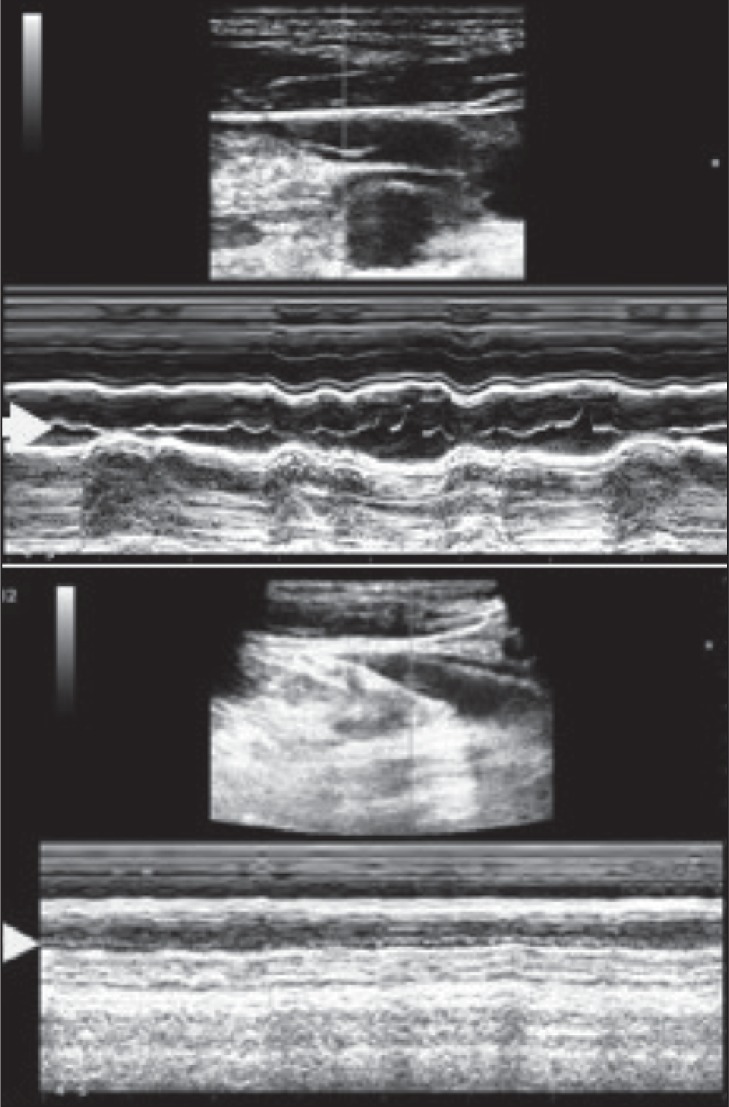
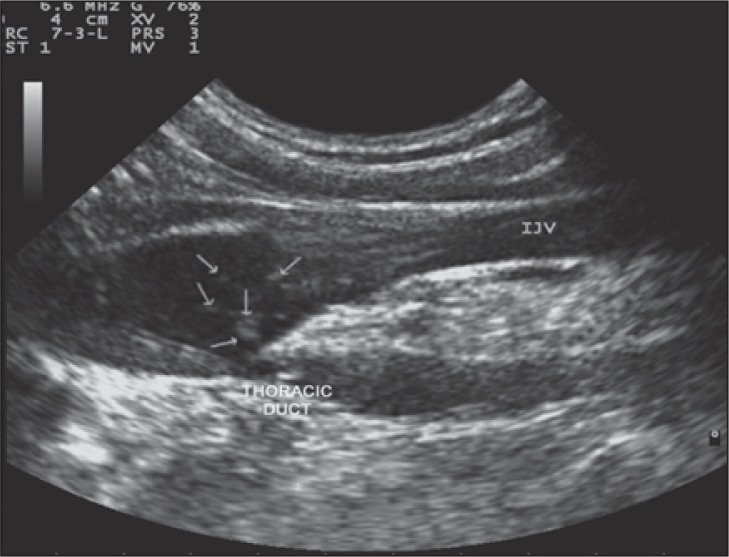
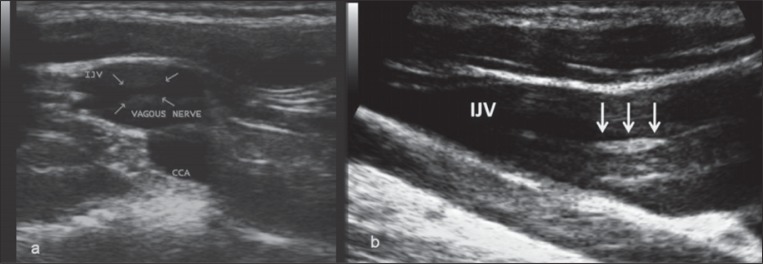
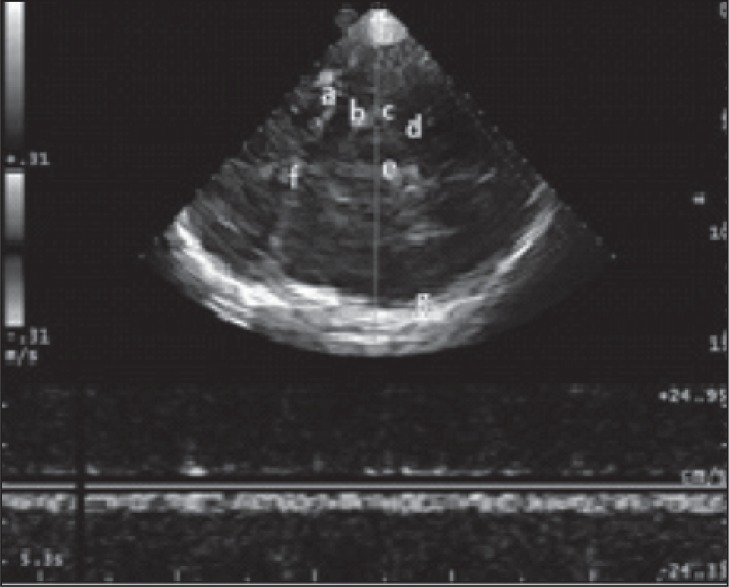
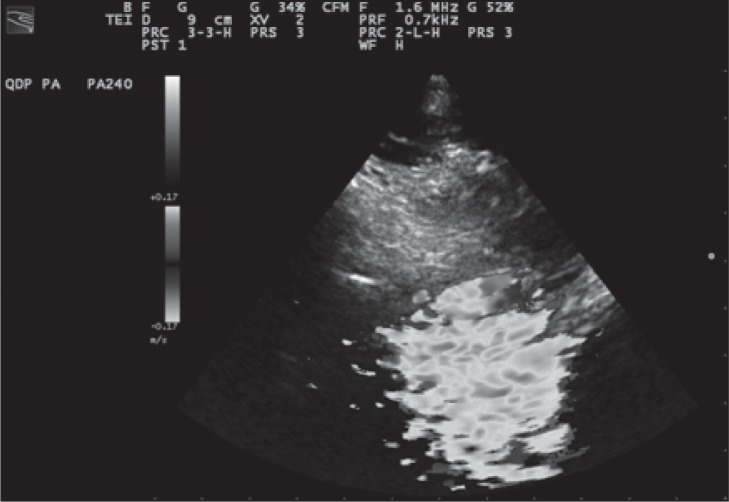
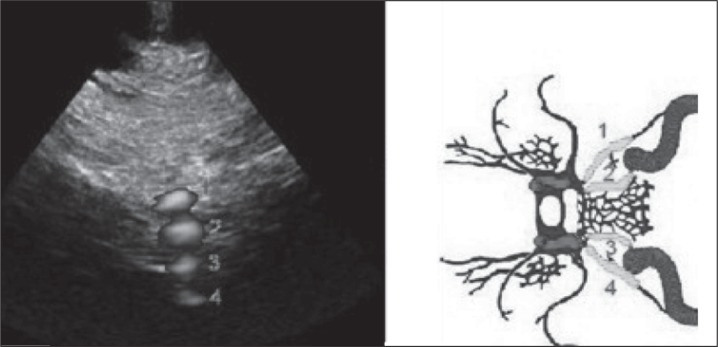
Chronic cerebrospinal venous insufficiency (CCSVI) is a syndrome characterized by stenoses or obstructions of the internal jugular and/or azygos veins with disturbed flow and formation of collateral venous channels. Ultrasound and venographic studies of the internal jugular and azygos venous systems in patients with multiple sclerosis (MS) have demonstrated a high prevalence of CCSVI (mean 71%, range 0-100%; n=1336) associated with activation of collaterals. By contrast, ultrasound and venographic examinations of normal controls and patients without MS have demonstrated a much lower prevalence (mean 7.1%, range 0-22%; n=505). Ultrasound in the form of duplex scanning uses a combination of physiological measurements as well as anatomical imaging and has been used for the detection of CCSVI by different centers with variable results. A high prevalence of obstructive lesions, ranging from 62% to 100%, has been found by some teams in patients with MS compared with a low prevalence (0-25%) in controls. However, others have reported absence of these lesions or a lower prevalence (16-52%). This variability could be the result of differences in technique, training, experience or criteria used. In order to ensure a high reproducibility of duplex scanning with comparable accuracy between centers a detailed protocol with standard methodology and criteria is needed. Also, standardization of the method of reporting of duplex measurements and other findings will facilitate validation of the proposed criteria by different centers. The aim of this document is to produce recommendations for such a protocol and indicate what future research is needed in order to address areas of uncertainty.
Figures
References
-
- Zamboni P , Consorti G , Galeotti R , et al. Venous collateral circulation of the extracranial cerebrospinal outflow routes . Curr Neurovasc Res . 2009 ; 6 : 204 – 212 . - PubMed
-
- Zivadinov R , Marr K , Cutter G , et al. Prevalence, sensitivity, and specificity of chronic cerebrospinal venous insufficiency in MS . Neurology . 2011 ; 77 : 138 – 144 . - PubMed
-
- Al-Omari MH , Rousan LA . Internal jugular vein morphology and hemodynamics in patients with multiple sclerosis . Int Angiol . 2010 ; 29 : 115 – 120 . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources