

Inductive, scaffold-based, regenerative medicine approach to reconstruction of the temporomandibular joint disk
- PMID: 22365981
- PMCID: PMC3368066
- DOI: 10.1016/j.joms.2011.12.030
Inductive, scaffold-based, regenerative medicine approach to reconstruction of the temporomandibular joint disk
Abstract
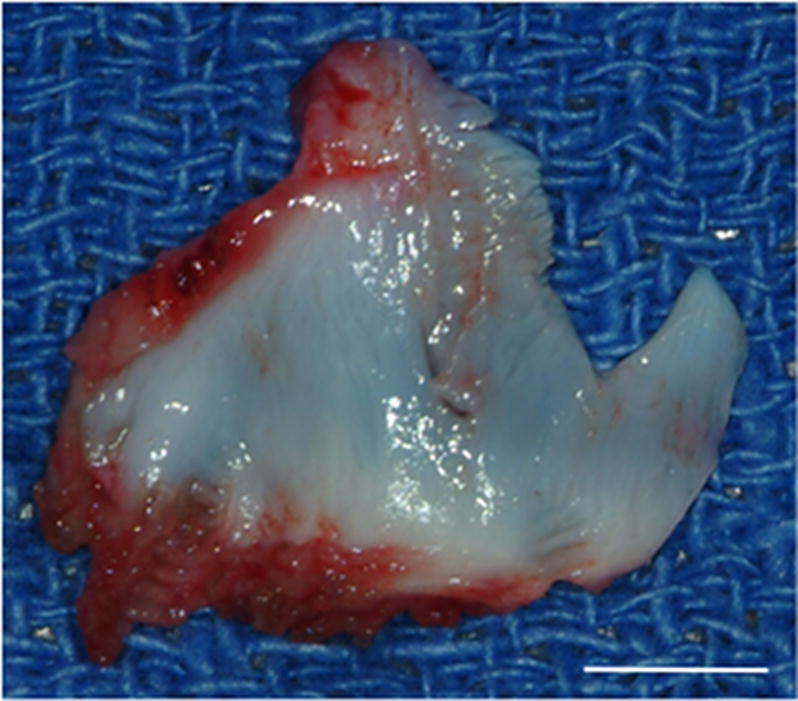
Purpose: A device composed of extracellular matrix (ECM) was investigated as an inductive template in vivo for reconstruction of the temporomandibular joint (TMJ) disk after discectomy.
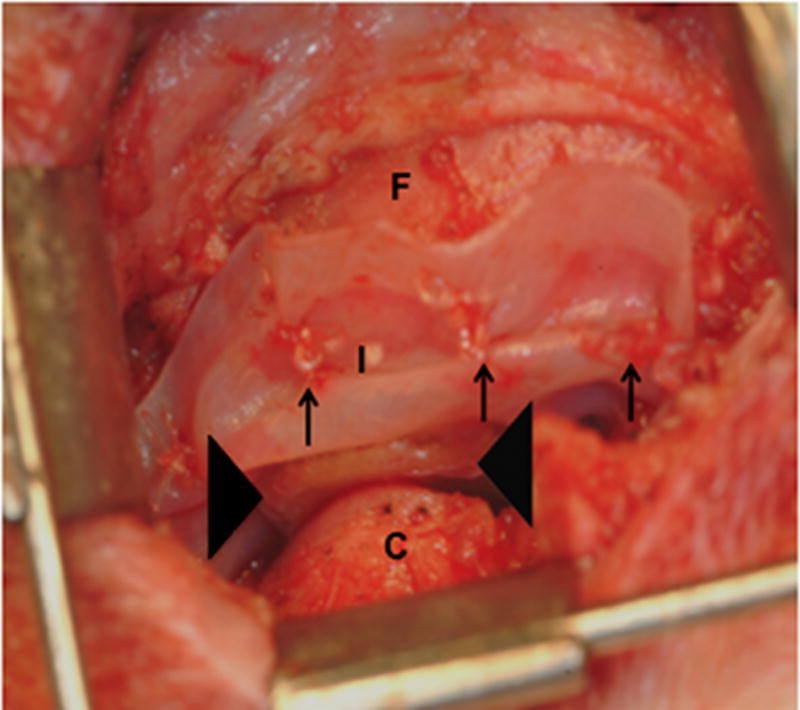
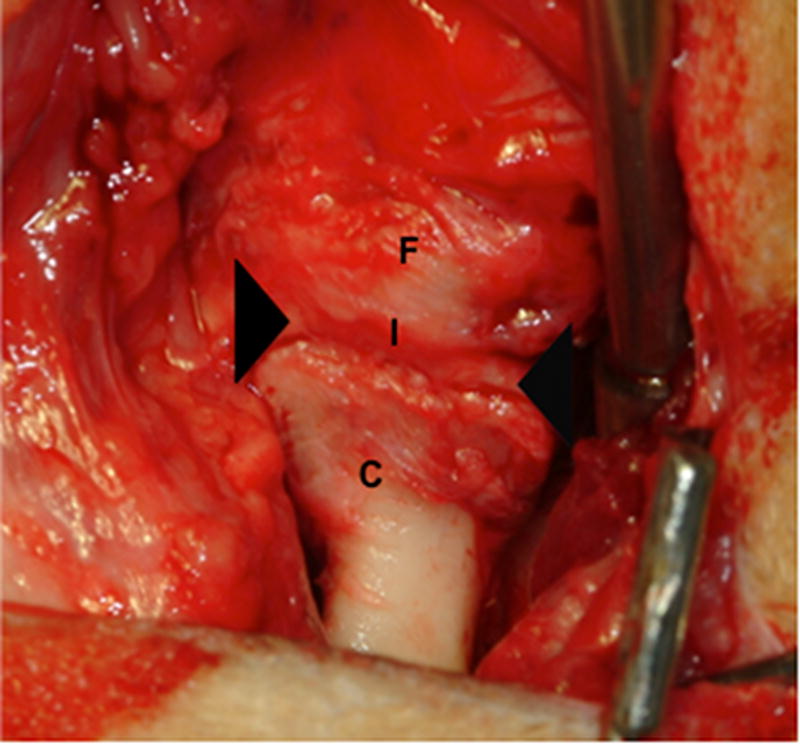
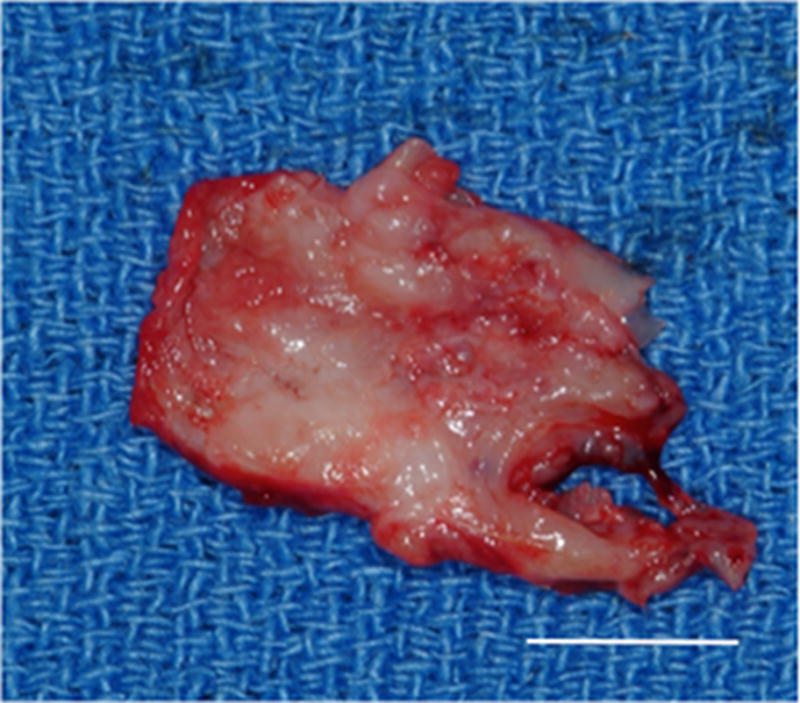
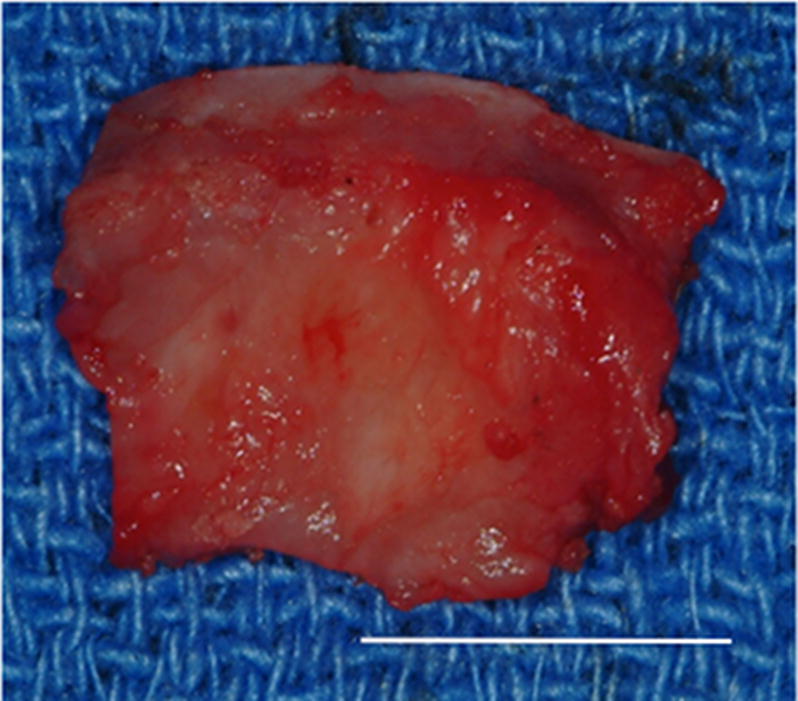
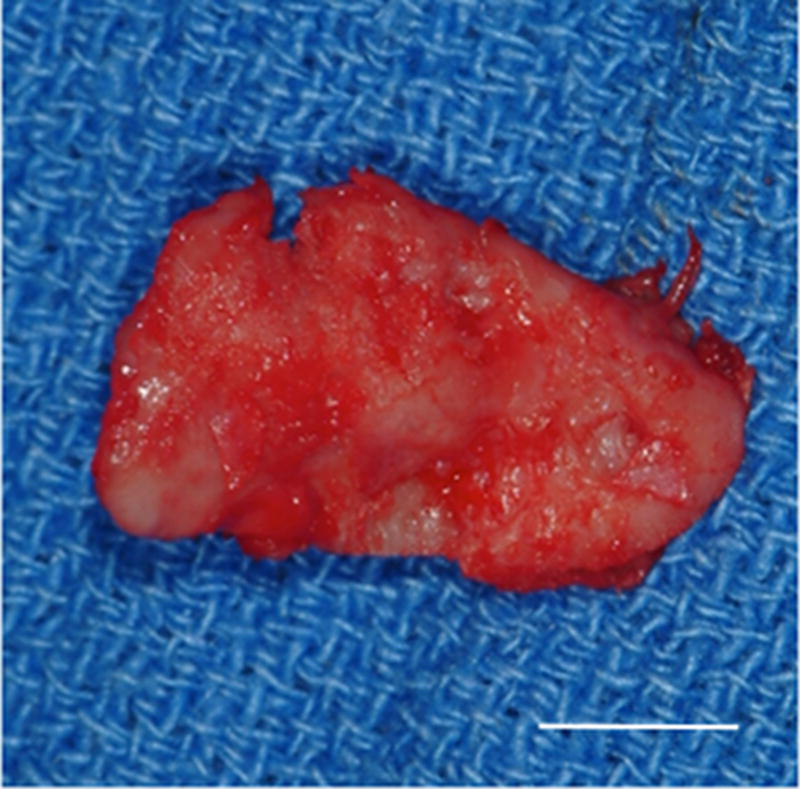
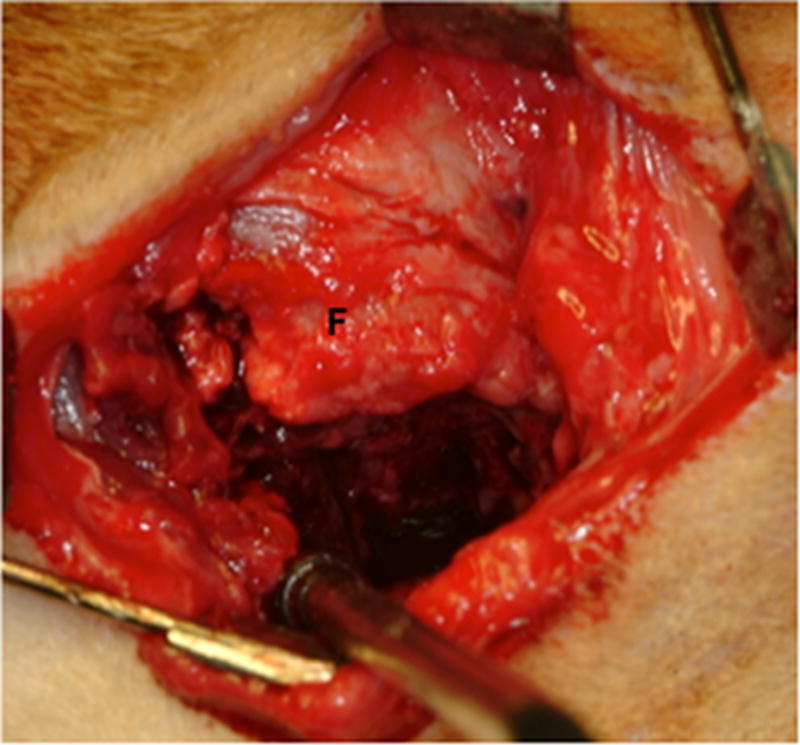
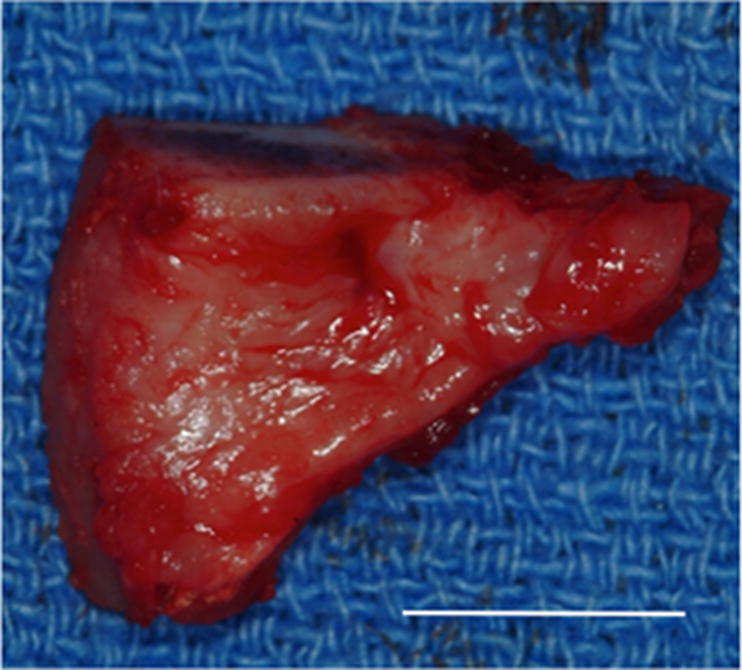
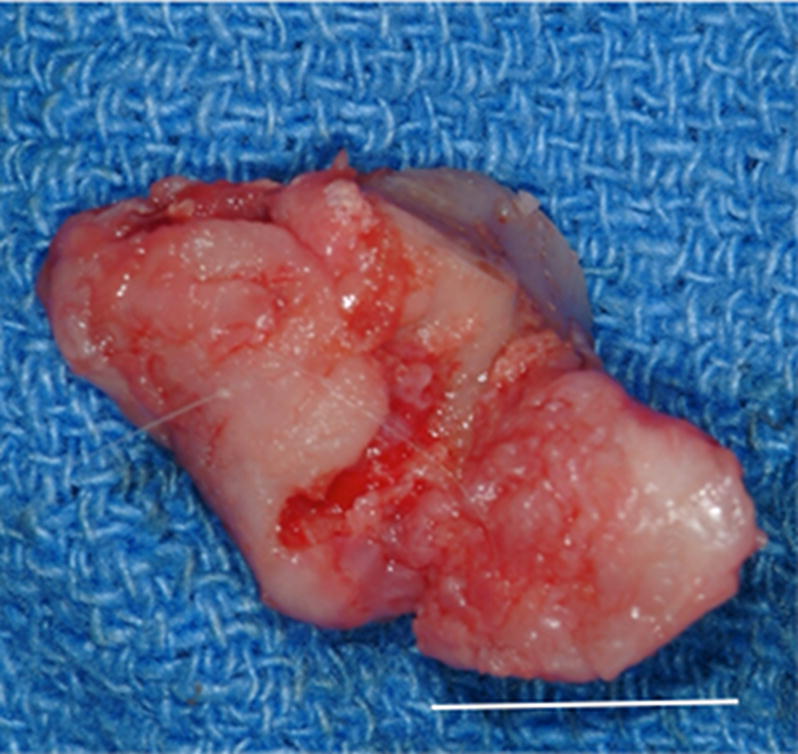
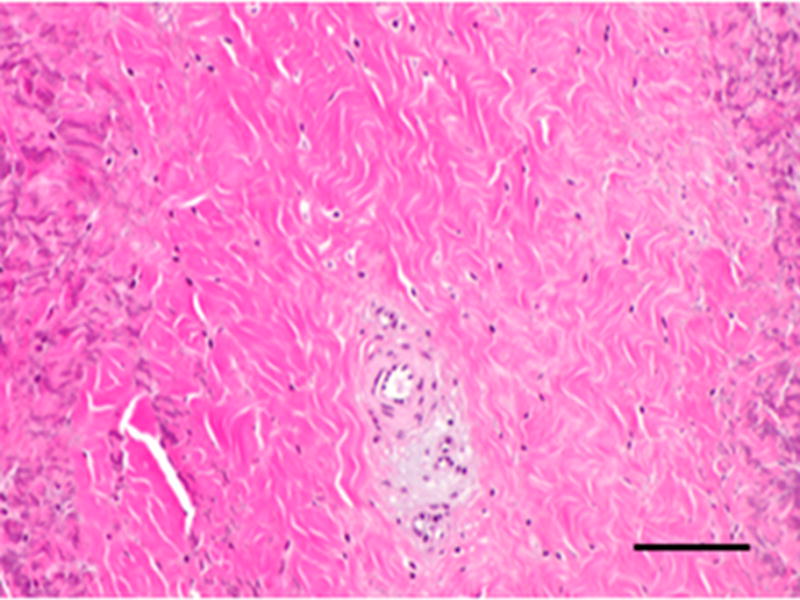
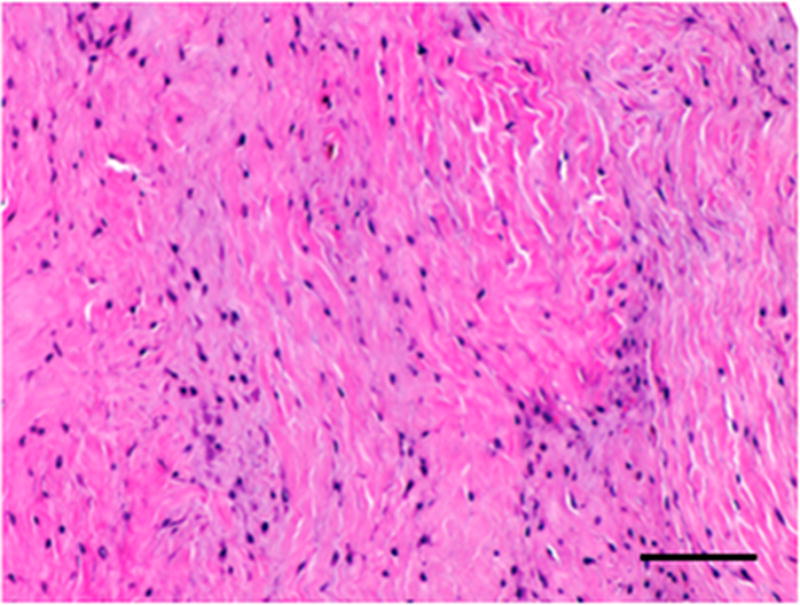
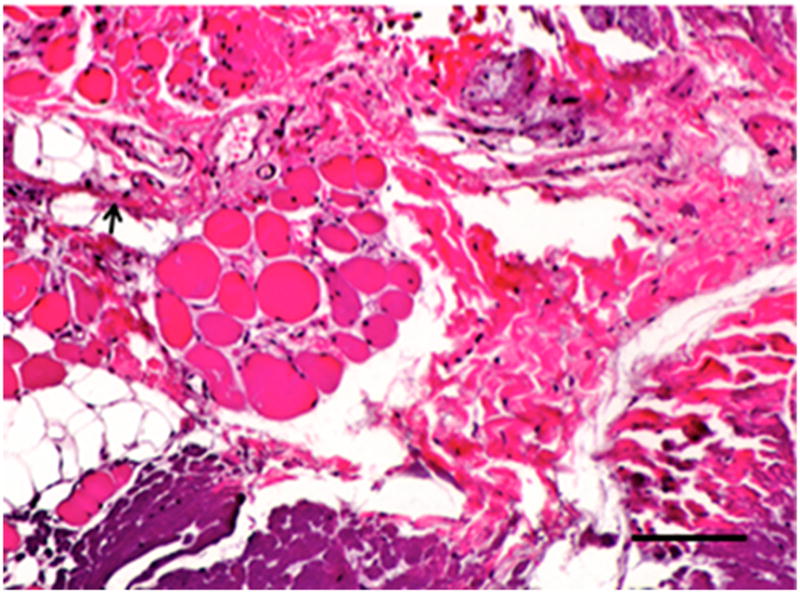
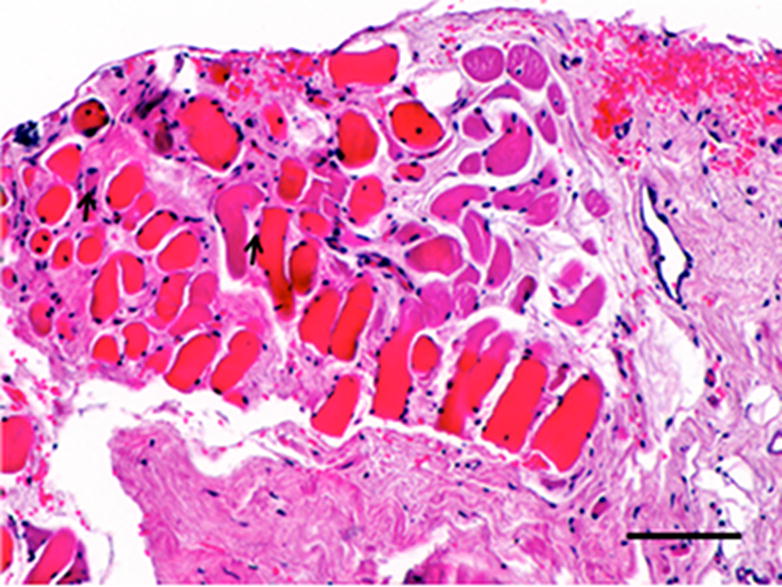
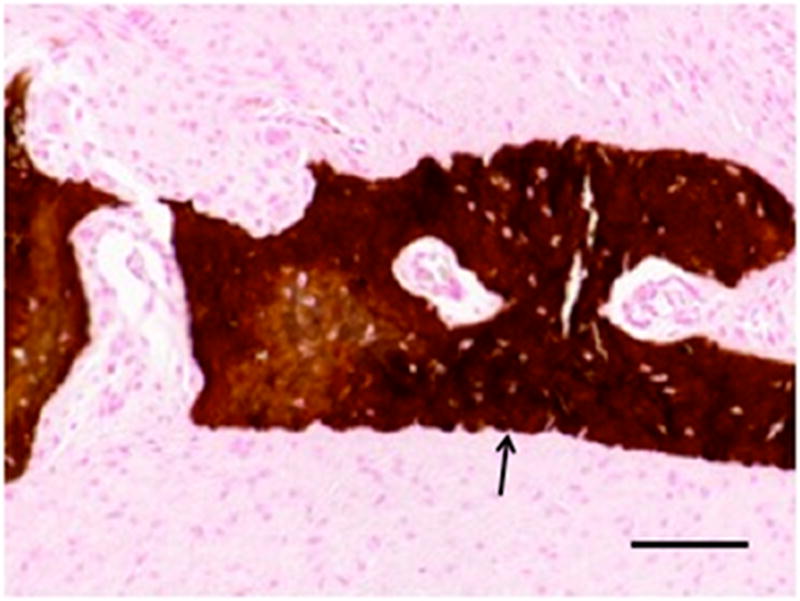
Materials and methods: A scaffold material composed of porcine-derived ECM was configured to mimic the shape and size of the TMJ. This device was implanted in a canine model of bilateral TMJ discectomy. After discectomy, 1 side was repaired with an ECM scaffold material and the contralateral side was left empty as a control. At 6 months after implantation, the joint space was opened, the joints were evaluated for signs of gross pathologic degenerative changes, and newly formed tissue was excised for histologic, biochemical, and biomechanical analysis.
Results: The results showed that implantation of an initially acellular material supported the formation of site-appropriate, functional host tissue that resembled that of the native TMJ disk. Furthermore, this prevented gross degenerative changes in the temporal fossa and mandibular condyle. No tissue formation and mild to severe gross pathologic changes were observed in the contralateral controls.
Conclusions: These results suggest that an ECM-based bioscaffold could represent an off-the-shelf solution for TMJ disk replacement.
Copyright © 2012 American Association of Oral and Maxillofacial Surgeons. Published by Elsevier Inc. All rights reserved.
Figures


References
-
- Alonso A, Kaimal S, Look J, Swift J, Fricton J, Myers S, et al. A quantitative evaluation of inflammatory cells in human temporomandibular joint tissues from patients with and without implants. J Oral Maxillofac Surg. 2009;67:788–96. - PubMed
-
- Fricton JR, Look JO, Schiffman E, Swift J. Long-term study of temporomandibular joint surgery with alloplastic implants compared with nonimplant surgery and nonsurgcal rehabilitation for painful temporomandibular joint disc displacement. J Oral Maxillofac Surg. 2002;60:1400–11. discussion 11-2. - PubMed
-
- Dolwick MF, Aufdemorte TB. Silicone-induced foreign body reaction and lymphadenopathy after temporomandibular join arthroplasty. Oal Surg Oral Medtroral Pathol. 1985;59:449–52. - PubMed
-
- Dimitroulis G. A critical review of interpositional grafts following temporomandibular joint discectomy with an overview of the dermis-fat graft. Int J Oral Maxillofac Surg. 2011;40:561–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
