

Airflow obstruction, lung function, and risk of incident heart failure: the Atherosclerosis Risk in Communities (ARIC) study
- PMID: 22366234
- PMCID: PMC3530346
- DOI: 10.1093/eurjhf/hfs016
Airflow obstruction, lung function, and risk of incident heart failure: the Atherosclerosis Risk in Communities (ARIC) study
Abstract
Aims: We examined the relationship between forced expiratory volume in 1 s (FEV(1)), airflow obstruction, and incident heart failure (HF) in black and white, middle-aged men and women in four US communities.
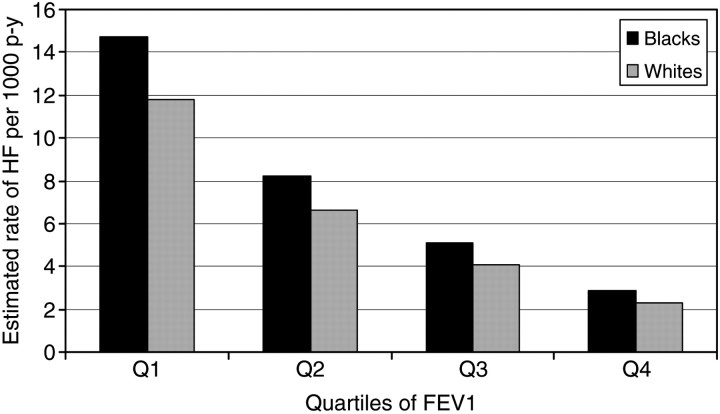
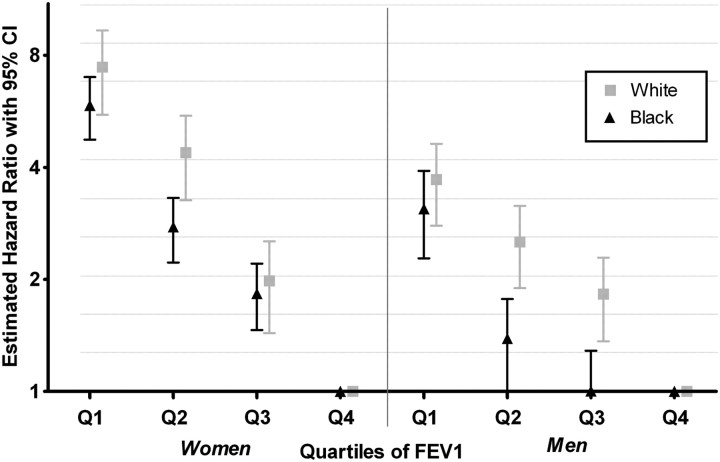
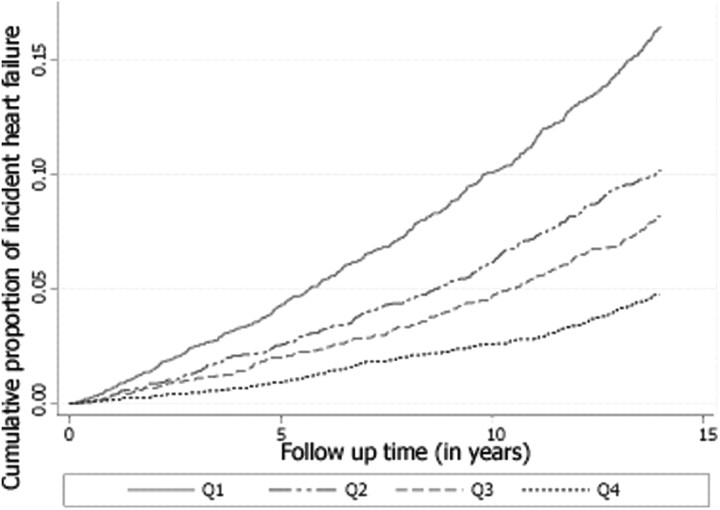
Methods and results: Lung volumes by standardized spirometry and information on covariates were collected on 15 792 Atherosclerosis Risk in Communities (ARIC) cohort participants in 1987-89. Incident HF was ascertained from hospital records and death certificates up to 2005 in 13 660 eligible participants. Over an average follow-up of 14.9 years, 1369 (10%) participants developed new-onset HF. The age- and height-adjusted hazard ratios (HRs) for HF increased monotonically over descending quartiles of FEV(1) for both genders, race groups, and smoking status. After multivariable adjustment for traditional cardiovascular risk factors and height, the HRs [95% confidence intervals (CIs)] of HF comparing the lowest with the highest quartile of FEV(1) were 3.91 (2.40-6.35) for white women, 3.03 (2.12-4.33) for white men, 2.11 (1.33-3.34) for black women, and 2.23 (1.37-3.59) for black men. The association weakened but remained statistically significant after additional adjustment for systemic markers of inflammation. The multivariable adjusted incidence of HF was higher in those with FEV(1)/forced vital capacity <70% vs. ≥70%: HR 1.44 (95% CI 1.20-1.74) among men and 1.40 (1.13-1.72) among women. A consistent and positive association with HF was seen for self-reported diagnosis of emphysema and chronic obstructive pulmonary disease, but not for asthma.
Conclusions: In this large population-based cohort with long-term follow-up, low FEV(1) and an obstructive respiratory disease were strongly and independently associated with the risk of incident HF.
Figures
Comment in
-
Chronic obstructive pulmonary disease: a slowly progressive cardiovascular disease masked by its pulmonary effects?Eur J Heart Fail. 2012 Apr;14(4):348-50. doi: 10.1093/eurjhf/hfs022. Epub 2012 Feb 25. Eur J Heart Fail. 2012. PMID: 22366235 No abstract available.
References
-
- Rosamond W, Flegal K, Furie K, Go A, Greenlund K, Haase N, Hailpern SM, Ho M, Howard V, Kissela B, Kittner S, Lloyd-Jones D, McDermott M, Meigs J, Moy C, Nichol G, O'Donnell C, Roger V, Sorlie P, Steinberger J, Thom T, Wilson M, Hong Y. Heart disease and stroke statistics—2008 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2008;117:e25–e146. - PubMed
-
- Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 2001;163:1256–1276. - PubMed
-
- Rutten FH, Cramer MJ, Lammers JW, Grobbee DE, Hoes AW. Heart failure and chronic obstructive pulmonary disease: an ignored combination? Eur J Heart Fail. 2006;8:706–711. - PubMed
-
- Sin DD, Wu L, Man SF. The relationship between reduced lung function and cardiovascular mortality: a population-based study and a systematic review of the literature. Chest. 2005;127:1952–1959. - PubMed
-
- Yilmaz R, Gencer M, Ceylan E, Demirbag R. Impact of chronic obstructive pulmonary disease with pulmonary hypertension on both left ventricular systolic and diastolic performance. J Am Soc Echocardiogr. 2005;18:873–881. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
