

Native nephrectomy prior to pediatric kidney transplantation: biological and clinical aspects
- PMID: 22366876
- PMCID: PMC3362721
- DOI: 10.1007/s00467-012-2115-y
Native nephrectomy prior to pediatric kidney transplantation: biological and clinical aspects
Abstract
Background: Pre-transplant nephrectomy is performed to reduce risks to graft and recipient. The aims of this study were to evaluate (1) indications, surgical approach, and morbidity of native nephrectomy and (2) the effects of kidney removal on clinical and biological parameters.
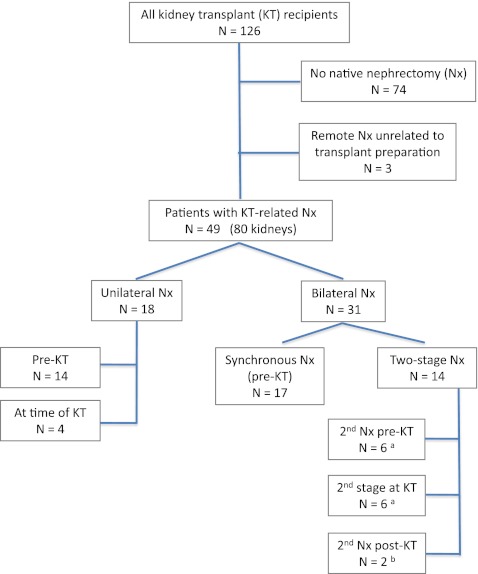
Methods: This study was designed as a single-center retrospective cohort study in which 49 consecutive patients with uni- or bilateral native nephrectomies were identified from a total of 126 consecutive graft recipients in our pediatric kidney transplantation database between 1992 and 2011. Demographic, clinical, and laboratory details were extracted from charts and electronic records, including operation reports and pre- and post-operative clinic notes.
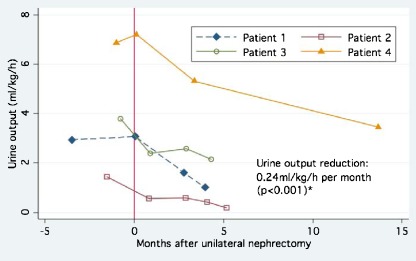
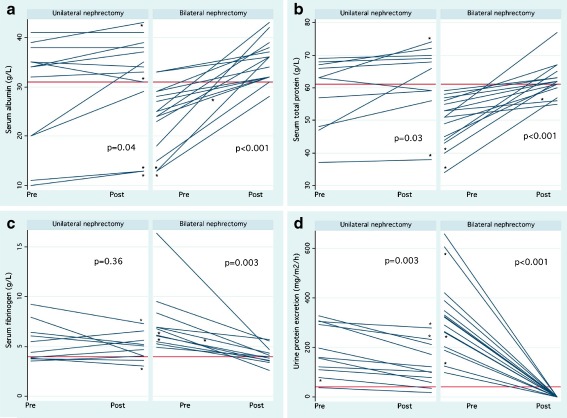
Results: Of the 49 nephrectomized patients, 47% had anomalies of the kidneys and urinary tract, 22% had cystinosis, 12% had focal segmental glomerulosclerosis, and 6% had congenital nephrotic syndrome. Nephrectomy decisions were based on clinical judgment, taking physiological and psychosocial aspects into consideration. Nephrectomy was performed in patients with polyuria (>2.5 ml/kg/h) and/or large proteinuria (>40 mg/m(2)/h), recurrent urinary tract infection or (rarely) hypertension. Urine output decreased from (median) 3.79 to 2.32 ml/kg/h (-34%), and proteinuria from 157 to 100 mg/m(2)/h (-40%) after unilateral nephrectomy (p=0.005). After bilateral nephrectomy, serum albumin, protein and fibrinogen concentrations normalized in 93, 73, and 55% of nephrectomized patients, respectively. Clinically relevant procedure-related complications (peritoneal laceration, hematoma) occurred in five patients.
Conclusion: In summary, we demonstrate quantitatively that native nephrectomy prior to transplantation improved serum protein levels and anticipated post-transplant fluid intake needs in select children, reducing the risk of graft hypoperfusion and its postulated consequences for graft outcome.
Figures
References
-
- Cochat P, Offner G. ESPN IV.11—Paediatrics (specific problems) Nephrol Dial Transplant. 2002;17:55–58. - PubMed
-
- Kerlin BA, Blatt NB, Fuh B, Zhao S, Lehman A, Blanchong C, Mahan JD, Smoyer WE. Epidemiology and risk factors for thromboembolic complications of childhood nephrotic syndrome: a Midwest Pediatric Nephrology Consortium (MWPNC) study. J Pediatr. 2009;155:105–110. doi: 10.1016/j.jpeds.2009.01.070. - DOI - PMC - PubMed
-
- Barbour SJ, Greenwald A, Djurdjev O, Levin A, Hladunewich MA, Nachman PH, Hogan SL, Cattran DC, Reich HN (2012) Disease-specific risk of venous thromboembolic events is increased in idiopathic glomerulonephritis. Kidney Int. 81(2):190–195 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
