

Trends in atrial fibrillation ablation: have we maximized the current paradigms?
- PMID: 22367051
- PMCID: PMC3396333
- DOI: 10.1007/s10840-011-9662-1
Trends in atrial fibrillation ablation: have we maximized the current paradigms?
Abstract
Purpose: The purpose of this study was to evaluate how atrial fibrillation (AF) ablation has evolved over time with regards to patient characteristics, procedural variables, complications, and outcomes.
Methods: We evaluated trends over time from 2003 to 2010 in clinical characteristics, procedural variables, complications, and Kaplan-Meier AF-free rates after the initial and final AF ablation in 1,125 patients undergoing 1,504 ablations.
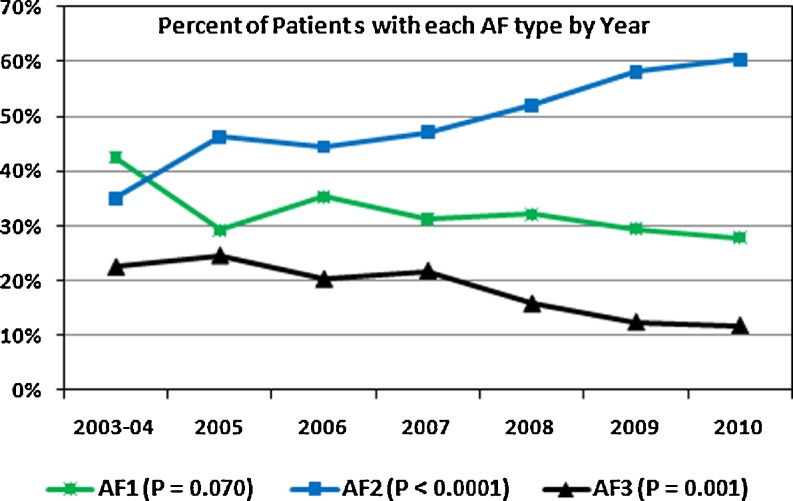
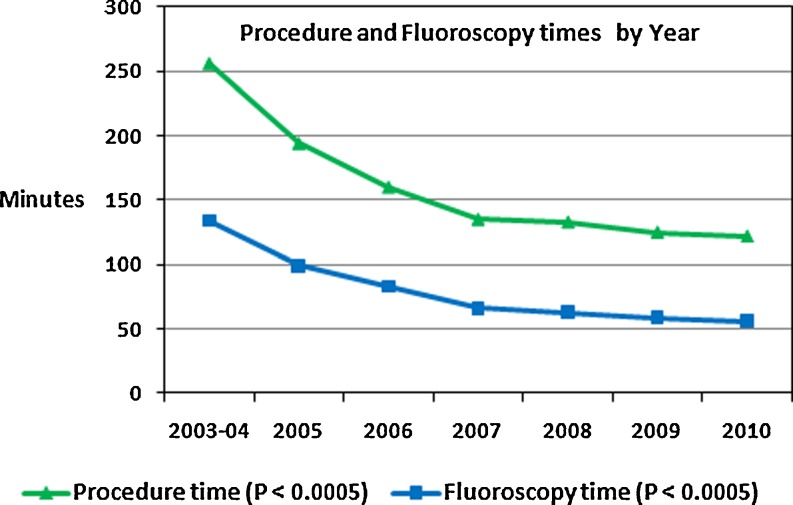
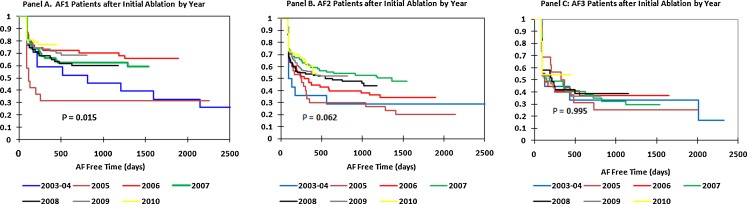
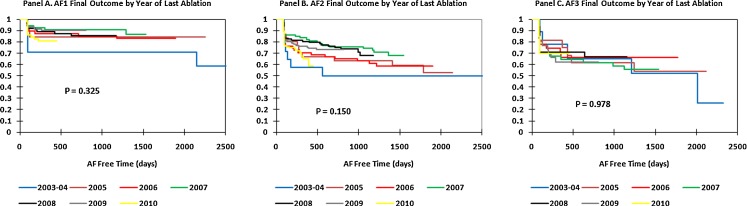
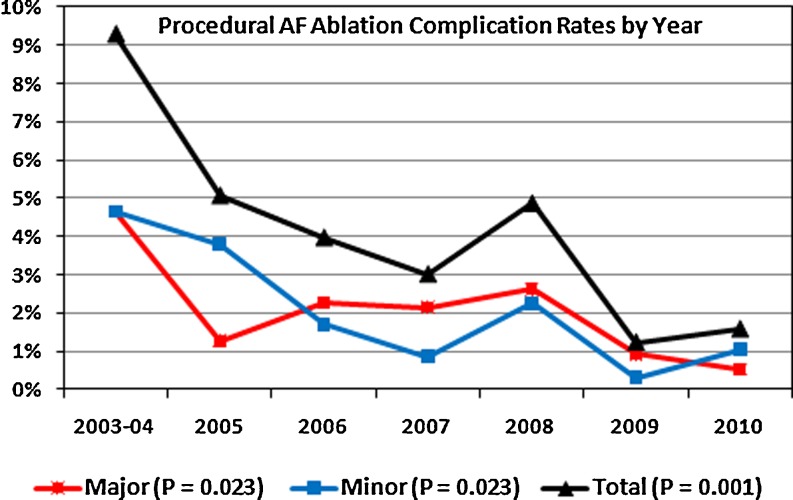
Results: Evaluating trends from 2003 to 2010, we found that patients undergoing AF ablation became older (P < 0.0001), had higher CHADS(2) scores (P < 0.0001), and more coronary artery disease (P = 0.021), persistent AF (P < 0.0001), hypertension (P < 0.0001), and previous strokes/transient ischemic attacks (P = 0.005). Procedure times decreased from 256 ± 49 to 122 ± 28 min (P < 0.0005), fluoroscopy times decreased from 134 ± 29 to 56 ± 19 min (P < 0.0005), and major (P = 0.023), minor (P = 0.023), and total complications (P = 0.001) decreased over time. The learning curve to minimize complications was 6 years. For paroxysmal AF, initial ablation AF-free rates improved over time (P = 0.015) but improvement plateaued in recent years. For persistent AF, initial ablation AF-free rates trended toward improvement over time (P = 0.062) but also plateaued in recent years. For long-standing persistent AF (P = 0.995), there was no outcome improvement after initial ablation over time. There was no trend for improved final outcomes (including repeat ablations) over time for paroxysmal, persistent, or long-standing AF (P = 0.150 to P = 0.978).
Conclusions: Despite decreased procedural and fluoroscopy times and reduced complication rates, post-ablation freedom from AF has not improved commensurately in recent years. A better understanding of AF initiation and maintenance may be required to devise personalized approaches to AF ablation and further improve outcomes.
Figures
Similar articles
-
Cryoballoon versus radiofrequency catheter ablation for paroxysmal atrial fibrillation.Pacing Clin Electrophysiol. 2015 Apr;38(4):483-9. doi: 10.1111/pace.12582. Epub 2015 Jan 28. Pacing Clin Electrophysiol. 2015. PMID: 25627795 Clinical Trial.
-
Five-year follow-up outcome after catheter ablation of persistent atrial fibrillation using a sequential biatrial linear defragmentation approach: What does atrial fibrillation termination during the procedure imply?Heart Rhythm. 2017 Jan;14(1):34-40. doi: 10.1016/j.hrthm.2016.08.041. Epub 2016 Aug 30. Heart Rhythm. 2017. PMID: 27590435
-
Impact of obesity on atrial fibrillation ablation: Patient characteristics, long-term outcomes, and complications.Heart Rhythm. 2017 Jun;14(6):819-827. doi: 10.1016/j.hrthm.2017.02.023. Epub 2017 Feb 20. Heart Rhythm. 2017. PMID: 28232261
-
Efficacy of ganglionated plexi ablation in addition to pulmonary vein isolation for paroxysmal versus persistent atrial fibrillation: a meta-analysis of randomized controlled clinical trials.J Interv Card Electrophysiol. 2017 Dec;50(3):253-260. doi: 10.1007/s10840-017-0285-z. Epub 2017 Sep 8. J Interv Card Electrophysiol. 2017. PMID: 28887742 Review.
-
Novel usage of the cryoballoon catheter to achieve large area atrial substrate modification in persistent and long-standing persistent atrial fibrillation.J Interv Card Electrophysiol. 2016 Sep;46(3):275-85. doi: 10.1007/s10840-016-0120-y. Epub 2016 Mar 3. J Interv Card Electrophysiol. 2016. PMID: 26936265 Review.
Cited by
-
Diagnosis-to-Ablation Time and Recurrence of Atrial Fibrillation Following Catheter Ablation: A Systematic Review and Meta-Analysis of Observational Studies.Circ Arrhythm Electrophysiol. 2020 Apr;13(4):e008128. doi: 10.1161/CIRCEP.119.008128. Epub 2020 Mar 19. Circ Arrhythm Electrophysiol. 2020. PMID: 32191539 Free PMC article.
-
Ablating persistent atrial fibrillation successfully.Curr Cardiol Rep. 2012 Oct;14(5):563-70. doi: 10.1007/s11886-012-0296-4. Curr Cardiol Rep. 2012. PMID: 22828755 Free PMC article. Review.
-
Internationally validated score to predict the outcome of non-paroxysmal atrial fibrillation ablation: the 'FLAME score'.Open Heart. 2021 Aug;8(2):e001653. doi: 10.1136/openhrt-2021-001653. Open Heart. 2021. PMID: 34348972 Free PMC article.
-
Theoretical considerations for mapping activation in human cardiac fibrillation.Chaos. 2013 Jun;23(2):023113. doi: 10.1063/1.4807098. Chaos. 2013. PMID: 23822478 Free PMC article.
-
Physician-controlled costs: the choice of equipment used for atrial fibrillation ablation.J Interv Card Electrophysiol. 2013 Mar;36(2):157-65. doi: 10.1007/s10840-013-9782-x. Epub 2013 Mar 14. J Interv Card Electrophysiol. 2013. PMID: 23483336 Free PMC article.
References
-
- Haissaguerre M, Jais P, Shah D, Takahashi A, Hocini M, Quiniou G, Garrigue S, Mouroux AL, Metayer PL, Clementy J. Spontaneous initiation of atrial fibrillation by ectopic beats originating from the pulmonary veins. The New England Journal of Medicine. 1998;339:659–666. doi: 10.1056/NEJM199809033391003. - DOI - PubMed
-
- Nademanee K, McKenzie J, Kosar E, Schwab M, Sunsaneewitayakul B, Vasavakul T, Khunnawat C, Ngarmukos T. A new approach for catheter ablation of atrial fibrillation: Mapping of the electrophysiologic substrate. Journal of the American College of Cardiology. 2004;43:2044–2053. doi: 10.1016/j.jacc.2003.12.054. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
