

Formalized prediction of clinically significant prostate cancer: is it possible?
- PMID: 22367181
- PMCID: PMC3720158
- DOI: 10.1038/aja.2011.140
Formalized prediction of clinically significant prostate cancer: is it possible?
Abstract
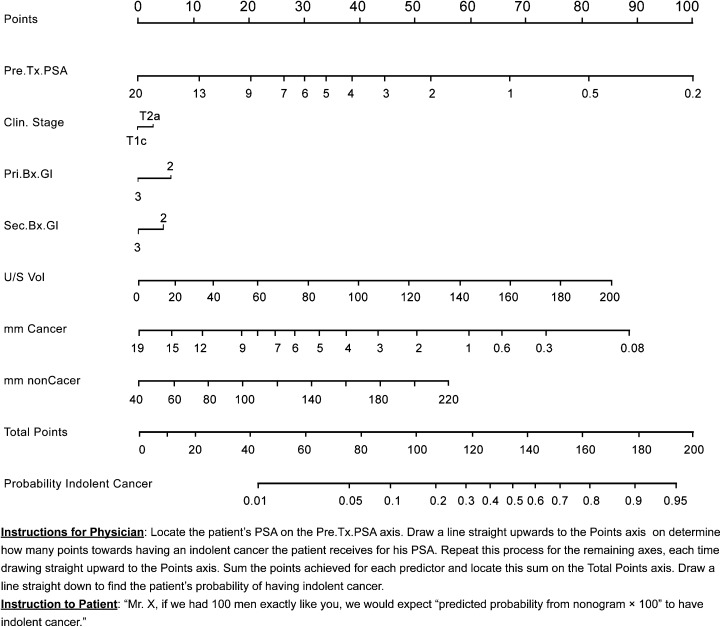
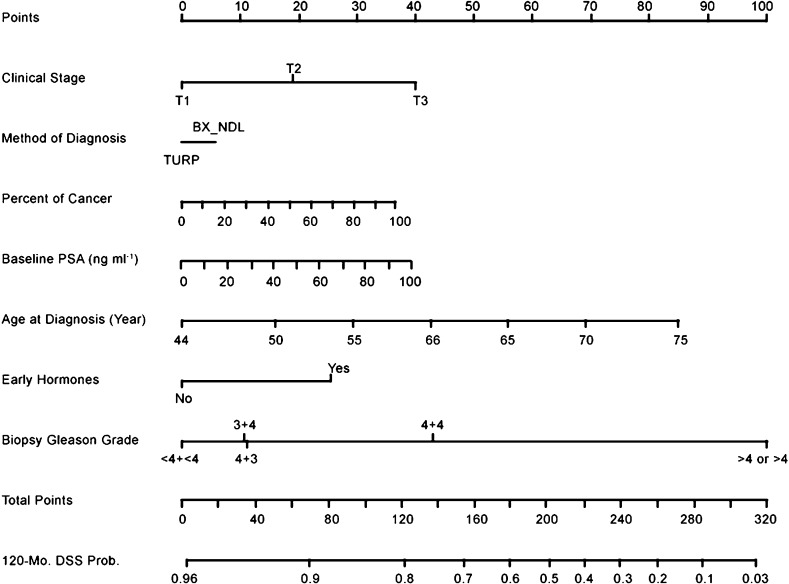
Greater understanding of the biology and epidemiology of prostate cancer in the last several decades have led to significant advances in its management. Prostate cancer is now detected in greater numbers at lower stages of disease and is amenable to multiple forms of efficacious treatment. However, there is a lack of conclusive data demonstrating a definitive mortality benefit from this earlier diagnosis and treatment of prostate cancer. It is likely due to the treatment of a large proportion of indolent cancers that would have had little adverse impact on health or lifespan if left alone. Due to this overtreatment phenomenon, active surveillance with delayed intervention is gaining traction as a viable management approach in contemporary practice. The ability to distinguish clinically insignificant cancers from those with a high risk of progression and/or lethality is critical to the appropriate selection of patients for surveillance protocols versus immediate intervention. This chapter will review the ability of various prediction models, including risk groupings and nomograms, to predict indolent disease and determine their role in the contemporary management of clinically localized prostate cancer.
Figures
References
-
- Catalona WJ, Smith DS, Ratliff TL, Basler JW. Detection of organ-confined prostate cancer is increased through prostate-specific antigen-based screening. JAMA. 1993;270:948–54. - PubMed
-
- Bill-Axelson A, Holmberg L, Ruutu M, Haggman M, Andersson SO, et al. Radical prostatectomy versus watchful waiting in early prostate cancer. N Engl J Med. 2005;352:1977–84. - PubMed
-
- Horner MJ, Ries LA, Krapcho M, Neyman N, Aminou R, et al. SEER Cancer Statistics Review, 1975–2006. BethesdaMD; National Cancer Institute; 2009;
-
- BethesdaMD; National Cancer Institute; 2011; General Information about Prostate Cancer.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
