

Muscle function, physical performance and body composition changes in men with prostate cancer undergoing androgen deprivation therapy
- PMID: 22367184
- PMCID: PMC3735097
- DOI: 10.1038/aja.2011.104
Muscle function, physical performance and body composition changes in men with prostate cancer undergoing androgen deprivation therapy
Abstract
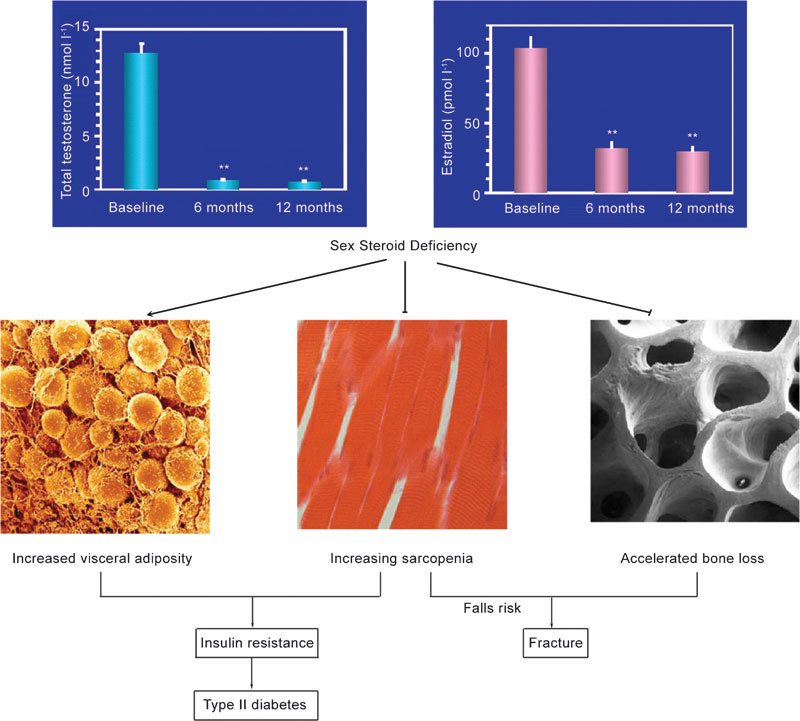
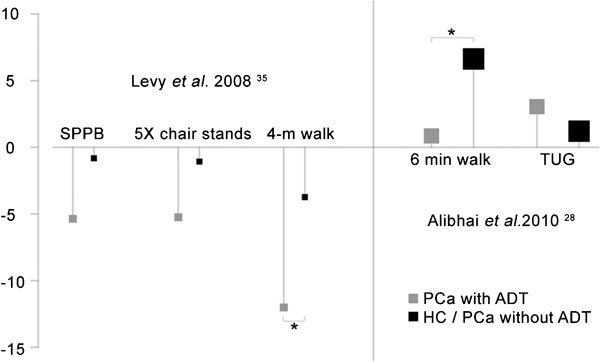
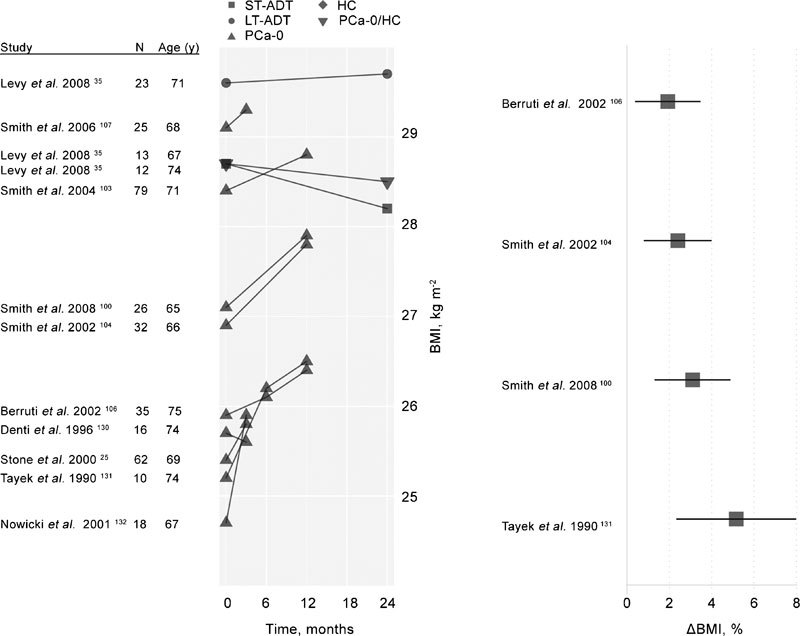
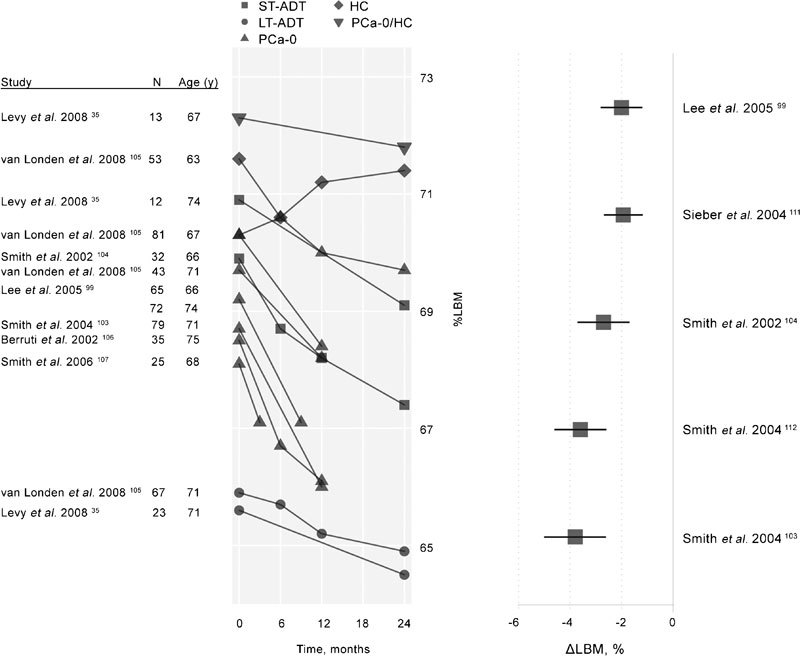
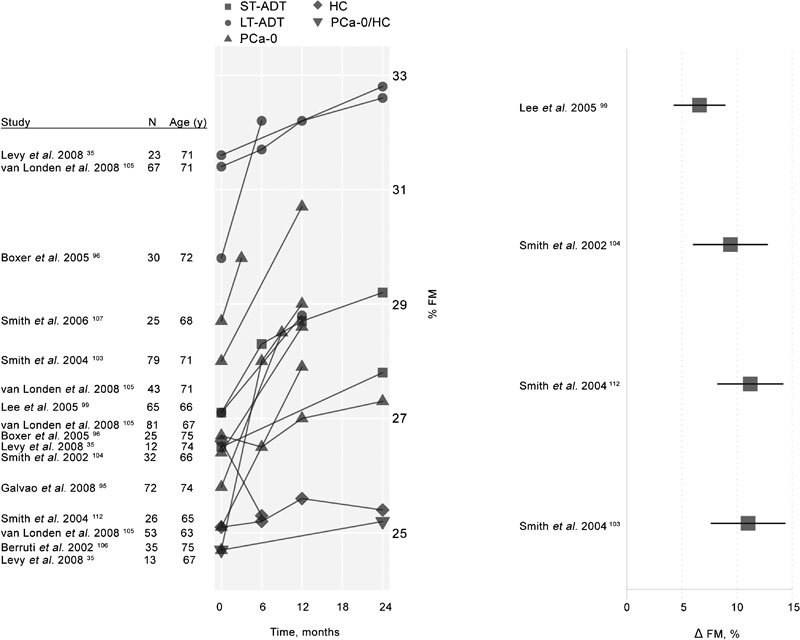
Prostate cancer (PCa) is the most common visceral malignancy in men with androgen deprivation therapy (ADT) the preferred therapy to suppress testosterone production and hence tumor growth. Despite its effectiveness in lowering testosterone, ADT is associated with side effects including loss of muscle mass, diminished muscle strength, decrements in physical performance, earlier fatigue and declining quality of life. This review reports a survey of the literature with a focus on changes in muscle strength, physical function and body composition, due to short-term and long-term ADT. Studies in these areas are sparse, especially well-controlled, prospective randomized trials. Cross-sectional and longitudinal data (up to 2 years) for men with PCa treated with ADT as well as patients with PCa not receiving ADT and age-matched healthy men are presented when available. Based on limited longitudinal data, the adverse effects of ADT on muscle function, physical performance and body composition occur shortly after the onset of ADT and tend to persist and worsen over time. Exercise training is a safe and effective intervention for mitigating these changes and initial guidelines for exercise program design for men with PCa have been published by the American College of Sports Medicine. Disparities in study duration, types of studies and other patient-specific variables such as time since diagnosis, cancer stage and comorbidities may all affect an understanding of the influence of ADT on health, physical performance and mortality.
Figures
References
-
- Stoch SA, Parker RA, Chen L, Bubley G, Ko YJ, et al. Bone loss in men with prostate cancer treated with gonadotropin-releasing hormone agonists. J Clin Endocrinol Metab. 2001;86:2787–91. - PubMed
-
- Smith MR. Therapy Insight: osteoporosis during hormone therapy for prostate cancer. Nat Clin Pract Urol. 2005;2:608–15; quiz 28. - PubMed
-
- Levine GN, D'Amico AV, Berger P, Clark PE, Eckel RH, et al. Androgen-deprivation therapy in prostate cancer and cardiovascular risk: a science advisory from the American Heart Association, American Cancer Society, and American Urological Association: endorsed by the American Society for Radiation Oncology. Circulation. 2010;121:833–40. - PMC - PubMed
-
- Nguyen PL, Je Y, Schutz FA, Hoffman KE, Hu JC, et al. Association of androgen deprivation therapy with cardiovascular death in patients with prostate cancer: a meta-analysis of randomized trials. JAMA. 2011;306:2359–66. - PubMed
-
- Mauras N, Hayes V, Welch S, Rini A, Helgeson K, et al. Testosterone deficiency in young men: marked alterations in whole body protein kinetics, strength, and adiposity. J Clin Endocrinol Metab. 1998;83:1886–92. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
