

Myocardial ischemia reperfusion injury: from basic science to clinical bedside
- PMID: 22368166
- PMCID: PMC3457795
- DOI: 10.1177/1089253211436350
Myocardial ischemia reperfusion injury: from basic science to clinical bedside
Abstract
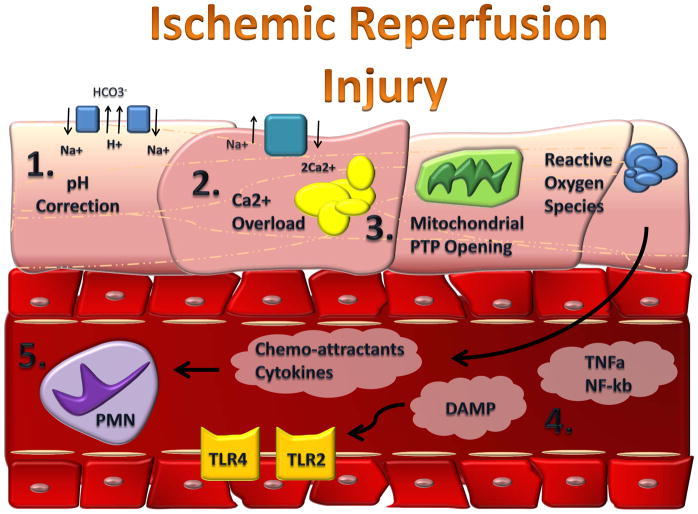
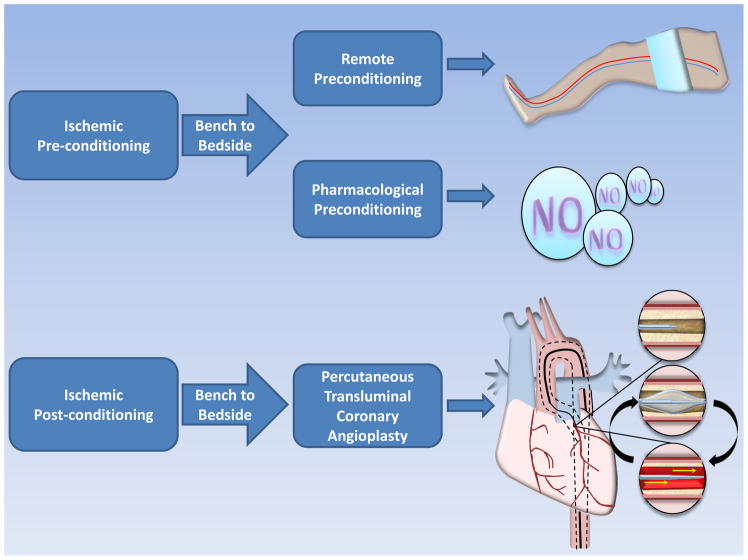
Myocardial ischemia reperfusion injury contributes to adverse cardiovascular outcomes after myocardial ischemia, cardiac surgery or circulatory arrest. Primarily, no blood flow to the heart causes an imbalance between oxygen demand and supply, named ischemia (from the Greek isch, restriction; and haema, blood), resulting in damage or dysfunction of the cardiac tissue. Instinctively, early and fast restoration of blood flow has been established to be the treatment of choice to prevent further tissue injury. Indeed, the use of thrombolytic therapy or primary percutaneous coronary intervention is the most effective strategy for reducing the size of a myocardial infarct and improving the clinical outcome. Unfortunately, restoring blood flow to the ischemic myocardium, named reperfusion, can also induce injury. This phenomenon was therefore termed myocardial ischemia reperfusion injury. Subsequent studies in animal models of acute myocardial infarction suggest that myocardial ischemia reperfusion injury accounts for up to 50% of the final size of a myocardial infarct. Consequently, many researchers aim to understand the underlying molecular mechanism of myocardial ischemia reperfusion injury to find therapeutic strategies ultimately reducing the final infarct size. Despite the identification of numerous therapeutic strategies at the bench, many of them are just in the process of being translated to bedside. The current review discusses the most striking basic science findings made during the past decades that are currently under clinical evaluation, with the ultimate goal to treat patients who are suffering from myocardial ischemia reperfusion-associated tissue injury.
Figures
References
-
- Jennings RB, Sommers HM, Smyth GA, Flack HA, Linn H. Myocardial necrosis induced by temporary occlusion of a coronary artery in the dog. Arch Pathol. 1960;70:68–78. - PubMed
-
- Murry CE, Jennings RB, Reimer KA. Preconditioning with ischemia: a delay of lethal cell injury in ischemic myocardium. Circulation. 1986;74:1124–36. - PubMed
-
- Kloner RA, Bolli R, Marban E, Reinlib L, Braunwald E. Medical and cellular implications of stunning, hibernation, and preconditioning: an NHLBI workshop. Circulation. 1998;97:1848–67. - PubMed
-
- Jennings RB, Reimer KA. The cell biology of acute myocardial ischemia. Annu Rev Med. 1991;42:225–46. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
