

Three-dimensional trans-esophageal Echocardiographic Evaluation of Atrial Septal Defects: A Pictorial Essay
- PMID: 22368571
- PMCID: PMC3232598
Three-dimensional trans-esophageal Echocardiographic Evaluation of Atrial Septal Defects: A Pictorial Essay
Abstract
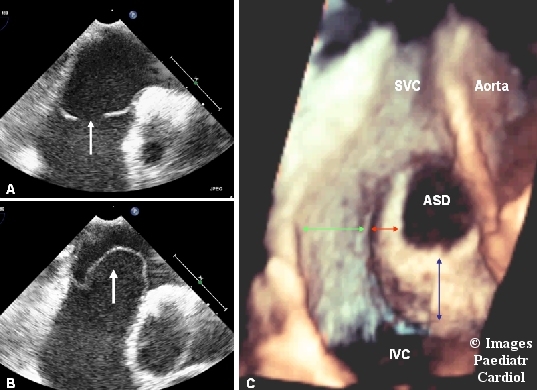
This pictorial assay illustrates the methodology of evaluating the atrial septal defects by three dimensional transesophageal echocardiography with the help of representative images. The article starts by discussing the technical details of how to acquire and crop the dataset to reconstruct the transesophageal three dimensional echocardiographic images of the inter atrial septum. Next, the anatomical details of the normal inter atrial septum are illustrated, followed by representative examples of all the possible defects of inter atrial septum. All the images have been reproduced in a uniform pattern which is similar to the view of the inter atrial septum that is seen in the real life situation by the surgeon.
Keywords: atrial septal defect; echocardiography.
Figures











Similar articles
-
Three-dimensional ultrasound imaging of the atrial septum: normal and pathologic anatomy.J Am Coll Cardiol. 1993 Nov 15;22(6):1673-8. doi: 10.1016/0735-1097(93)90594-q. J Am Coll Cardiol. 1993. PMID: 8227837
-
Transesophageal echocardiographic evaluation of atrial septal defects--how to explore the third dimension?Indian Heart J. 2009 Jul-Aug;61(4):328-34. Indian Heart J. 2009. PMID: 20635734
-
Three-dimensional transesophageal echocardiography of the atrial septal defects.Cardiovasc Ultrasound. 2008 Jul 18;6:38. doi: 10.1186/1476-7120-6-38. Cardiovasc Ultrasound. 2008. PMID: 18638394 Free PMC article.
-
Imaging the atrial septum using real-time three-dimensional transesophageal echocardiography: technical tips, normal anatomy, and its role in transseptal puncture.J Am Soc Echocardiogr. 2011 Jun;24(6):593-9. doi: 10.1016/j.echo.2011.01.022. Epub 2011 Mar 9. J Am Soc Echocardiogr. 2011. PMID: 21392940 Review.
-
Three-dimensional echocardiography of the atrial septum.Echocardiography. 2001 Jul;18(5):433-43. doi: 10.1046/j.1540-8175.2001.00433.x. Echocardiography. 2001. PMID: 11466156 Review.
Cited by
-
Assessment of Value of Three Dimensional Transesophageal Echocardiography versus Conventional Two Dimensional Transesophageal Echocardiography in Guiding Transcatheter Closure of Atrial Septal Defects and Patent Foramen Ovale.J Saudi Heart Assoc. 2022 Jul 6;34(1):85-99. doi: 10.37616/2212-5043.1303. eCollection 2022. J Saudi Heart Assoc. 2022. PMID: 35891893 Free PMC article.
References
-
- Rome JJ, Keane JF, Perry SB, Spevak PJ, Lock JE. Double umbrella closure of atrial defects.Initial clinical applications. Circulation. 1990;82:751–8. - PubMed
-
- Das GS, Voss G, Jarvis G, Wyche K, Gunther R, Wilson RF. Experimental atrial septal defect closure with a new, transcatheter, self-centering device. Circulation. 1993;88:1754–64. - PubMed
-
- Hellenbrand WE, Fahey JT, McGowan FX, Weltin GG, Kleinman CS. Transoesophageal echocardiographic guidance of transcatheter closure of atrial septal defect. Am J Cardiol. 1990;66:207–13. - PubMed
LinkOut - more resources
Full Text Sources