

Ventricular septal defects: morphology of the doubly committed juxtaarterial and muscular variants
- PMID: 22368583
- PMCID: PMC3232488
Ventricular septal defects: morphology of the doubly committed juxtaarterial and muscular variants
Abstract
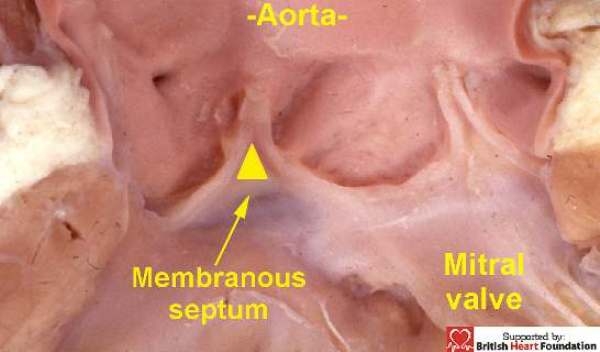
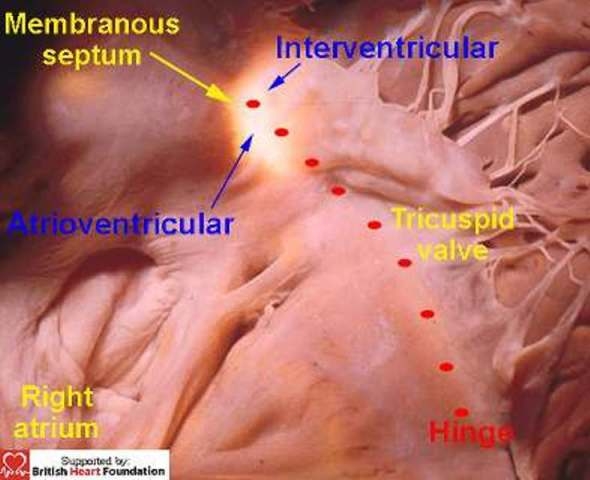
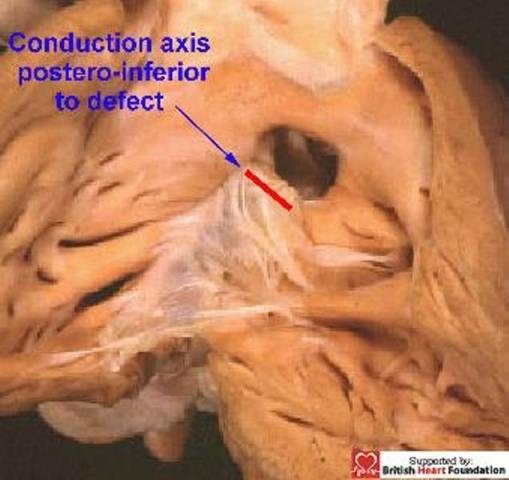
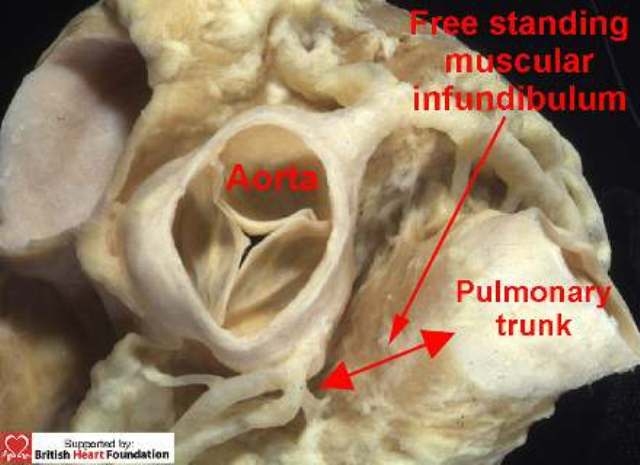
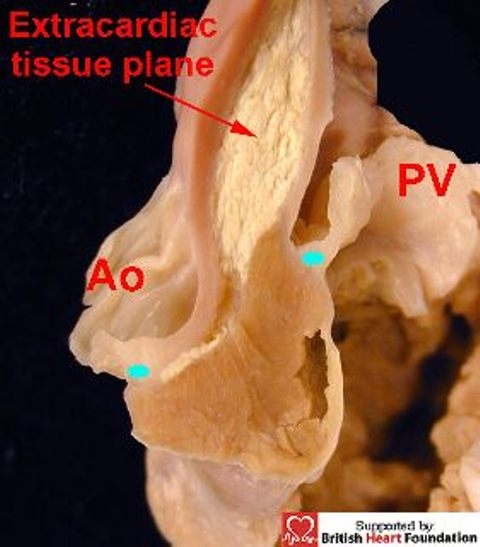
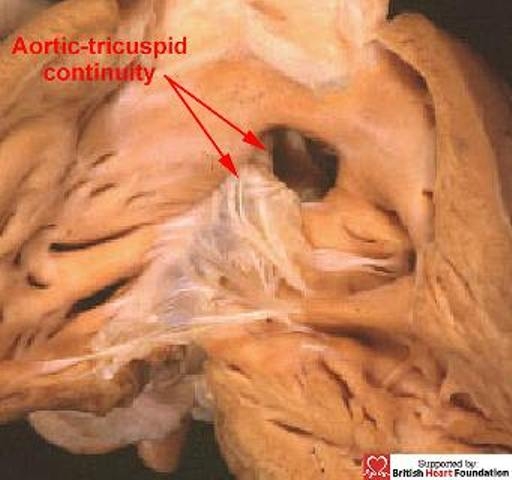
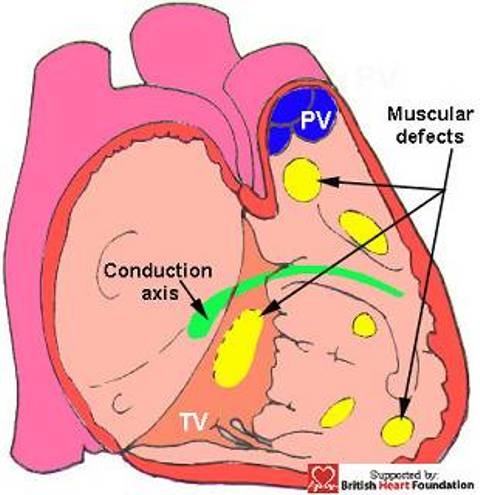
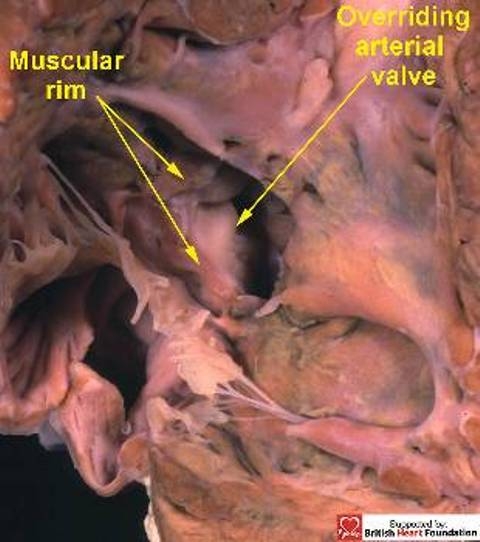
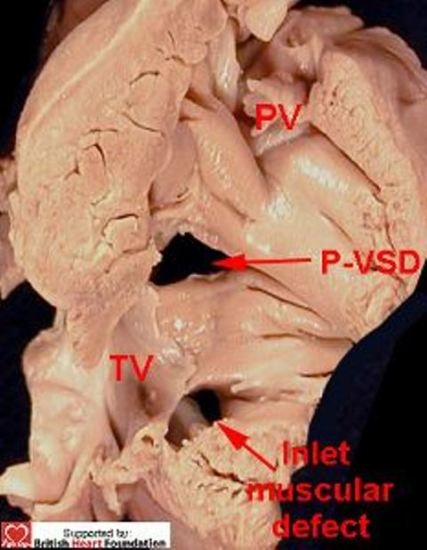
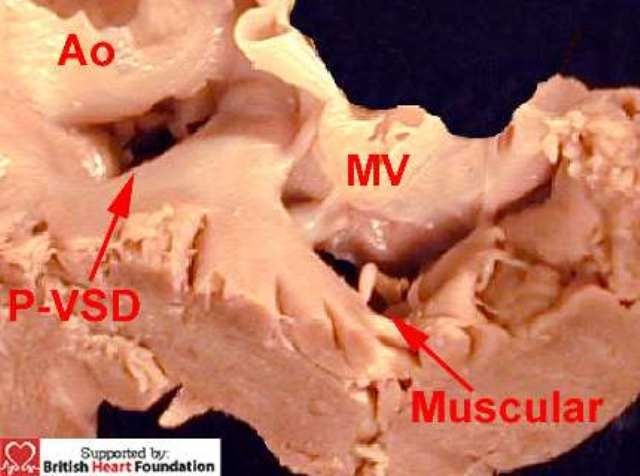
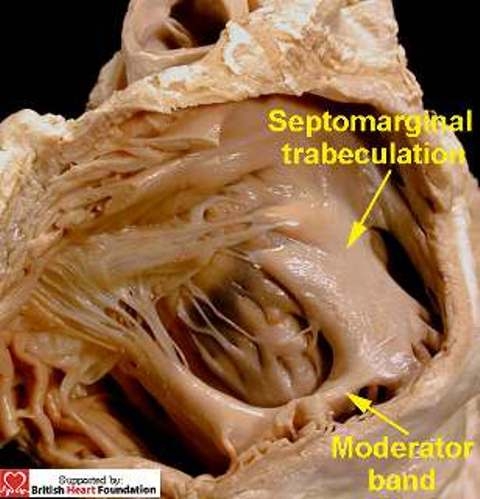
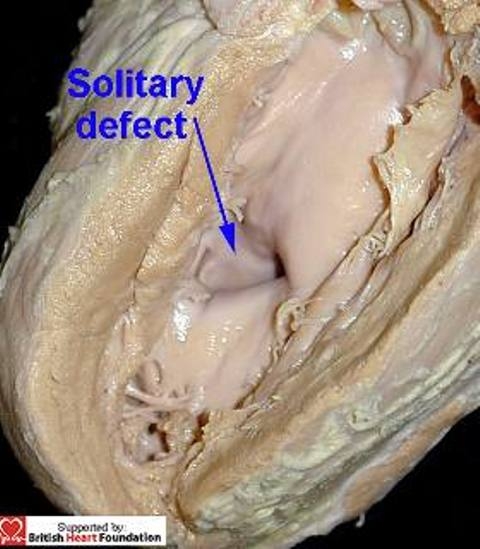
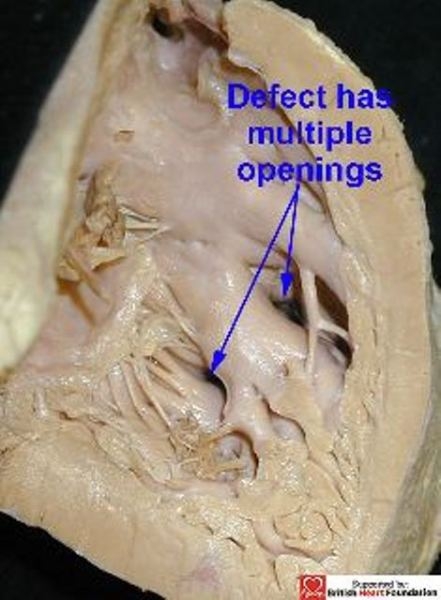
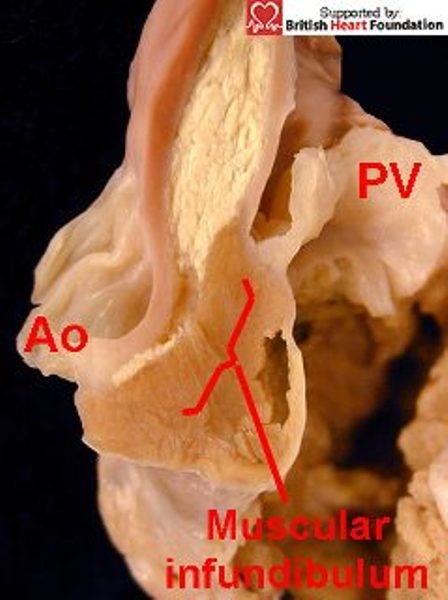
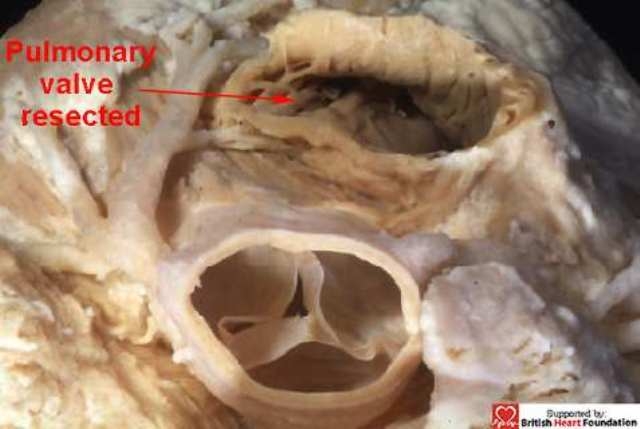
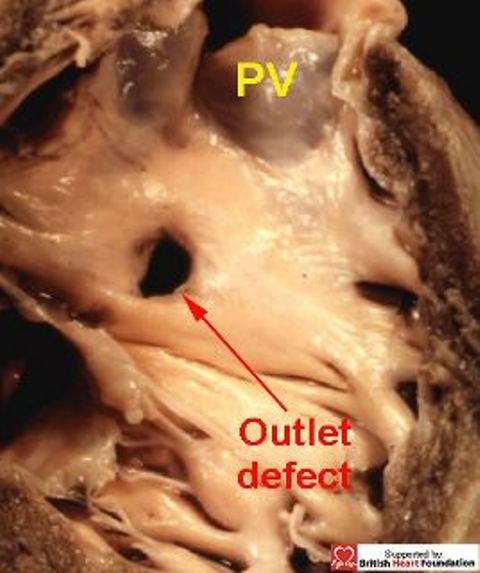
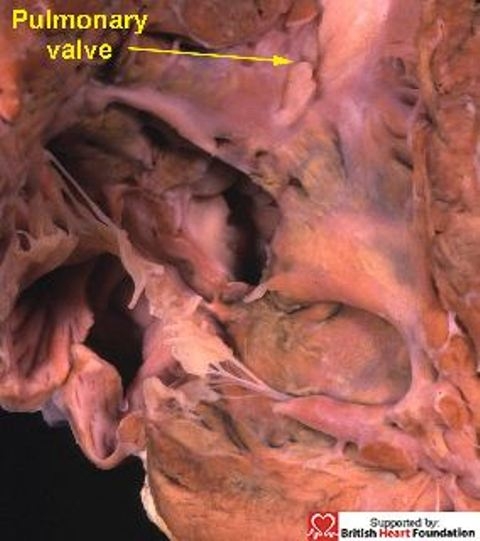
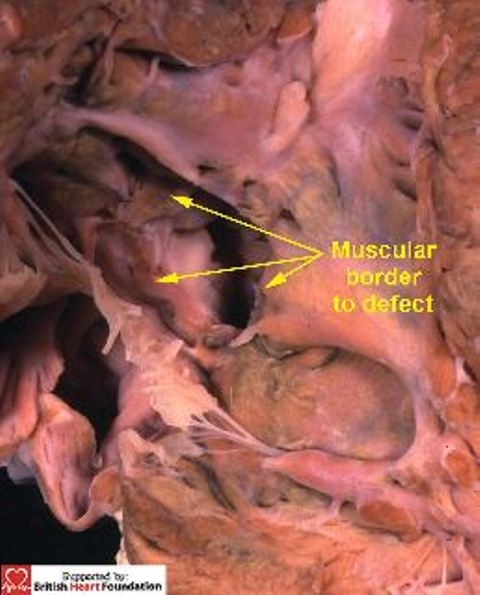
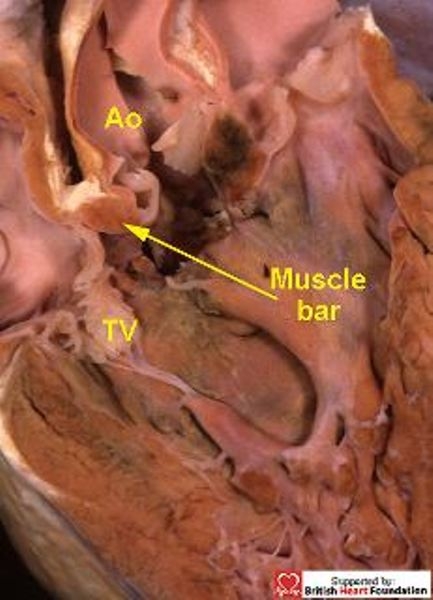
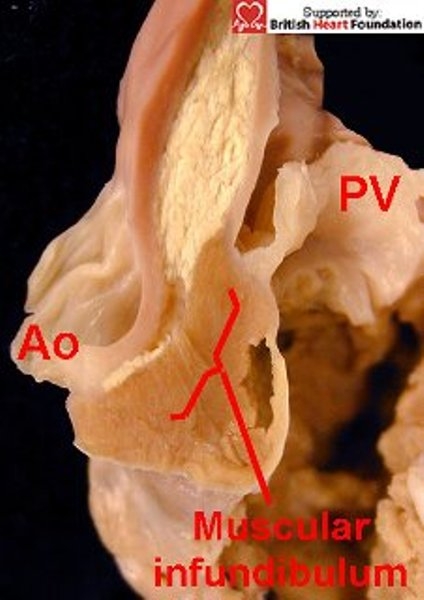
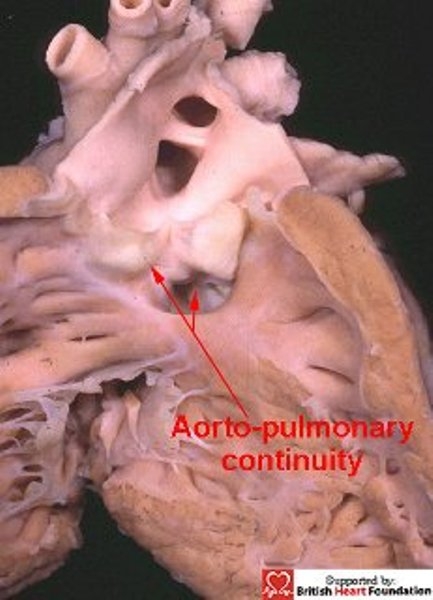
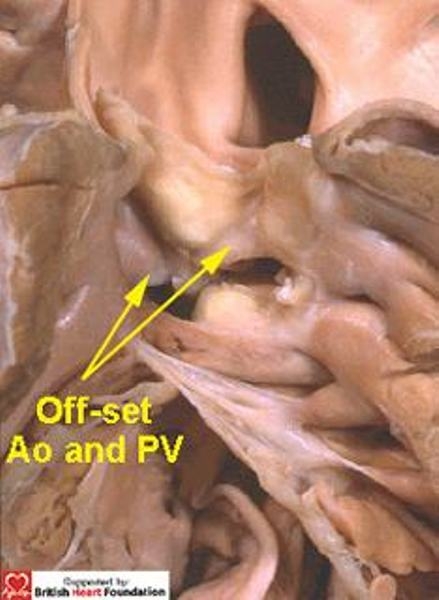
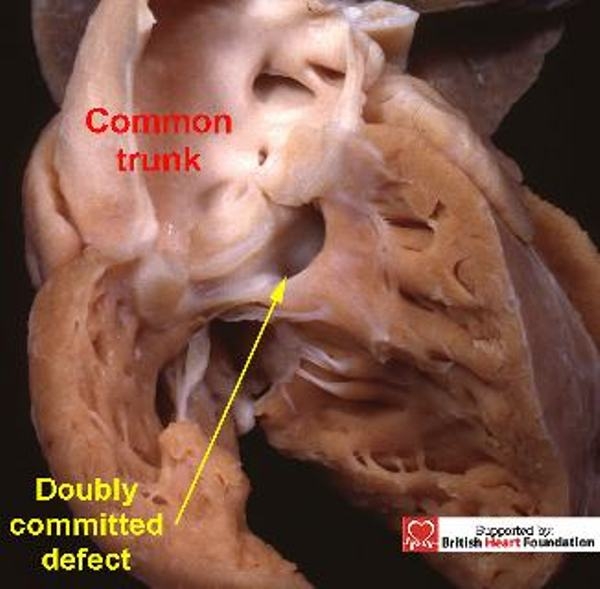
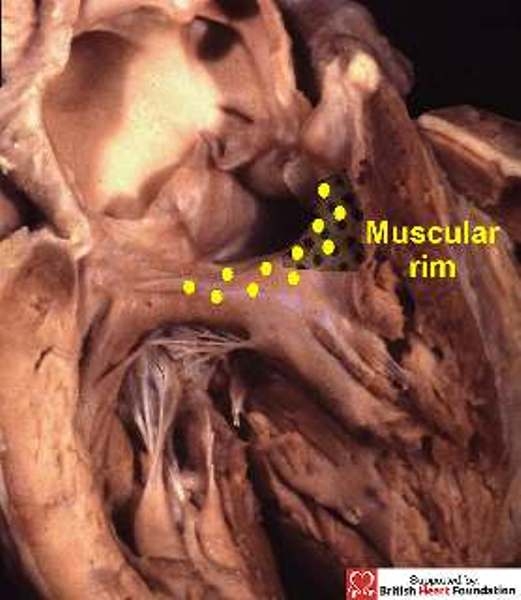
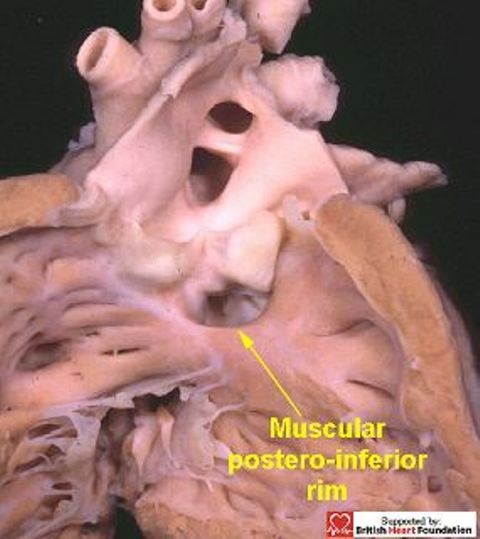
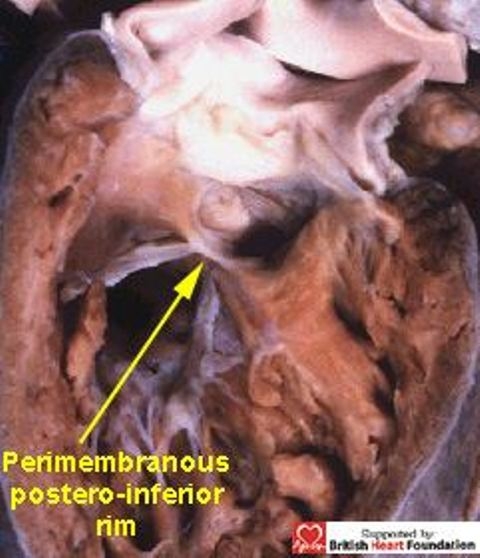
In our previous review of the phenotypic features of ventricular septal defects, we concentrated on the perimembranous variant, showing how its distinguishing feature, as viewed from the right ventricle, was fibrous continuity in its postero-inferior rim between the leaflets of the aortic and tricuspid valves. In this second review, we focus on the morphology of those defects which have exclusively muscular rims when viewed from their right side, and the variant with the phenotypic feature of fibrous continuity between the leaflets of the two arterial valves. As with the defects described as being perimembranous, once they have been characterised, it is the position of the defect relative to the components of the morphologically right ventricle that is the primary determinant of the options and strategies for treatment. Therefore, clarification of the morphology is the key to establishing the related risks for each particular defect.
Keywords: Heart defects; Heart septal defects; Heart ventricle/pathology; Heart ventricles/abnormalities; congenital; ventricular.
Figures




References
-
- McCarthy KP, Ho SY, Anderson RH. Categorisation of ventricular septal defects: review of the perimembranous morphology. Images Paediatr Cardiol. 2000;3:21–30. http://www.magnet.mt/health/impaedcard . - PMC - PubMed
-
- Franklin RCG, Anderson RH, Daniëls O, Elliott M, Gewillig MHML, Ghisla R, Krogman ON, Ulmer HE, Stocker FP. The European Paediatric Cardiac Code – The Short List. Cardiol Young. 2000;10(Suppl 1):8–26. - PubMed
-
- Franklin RCG. The European Paediatric Cardiac Code Long List: structure and function. Cardiol Young. 2000;10(Suppl 1):27–146. - PubMed
-
- Jacobs JP, Burke RP, Quintessenza JA, Mavroudis C. Congenital Heart Surgery Nomenclature and Database Project: ventricular septal defect. Ann Thorac Surg. 2000;69(Suppl 4):S25–35. - PubMed
-
- Anderson RH, Ho SY, Becker AE. Anatomy of the human atrioventricular junctions revisited. Anatomical Record. 2000;260:81–91. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials