

Prenatal diagnosis of congenital anomalies
- PMID: 22368596
- PMCID: PMC3232499
Prenatal diagnosis of congenital anomalies
Abstract
Up till the early 1970s, prenatal diagnosis of congenital anomalies was primarily aimed at detecting chromosomal abnormalities by amniocentesis.1. Over the last two decades, prenatal diagnosis has greatly benefited from advances in ultrasound technology and in our ability to detect microscopic and submicroscopic chromosome abnormalities as well as single gene disorders, leading to substantive improvements in detection of such congenital anomalies.2 At present, invasive prenatal diagnosis continues to be the gold standard for pregnancies at increased risk for chromosomal anomaly or other genetic disease, with chorionic villus sampling being the procedure of choice for the first trimester,3 whereas mid-trimester amniocentesis continues to be the most common form of invasive procedure for prenatal diagnosis.4 Still, invasive techniques are restricted to subgroups at risk for anomalies, for whom such time-consuming procedures are believed to be cost-effective, also accounting for procedure-related abortive risks. In the low-risk population prenatal diagnosis generally consists of screening procedures by means of ultrasound and maternal serum biochemistry.
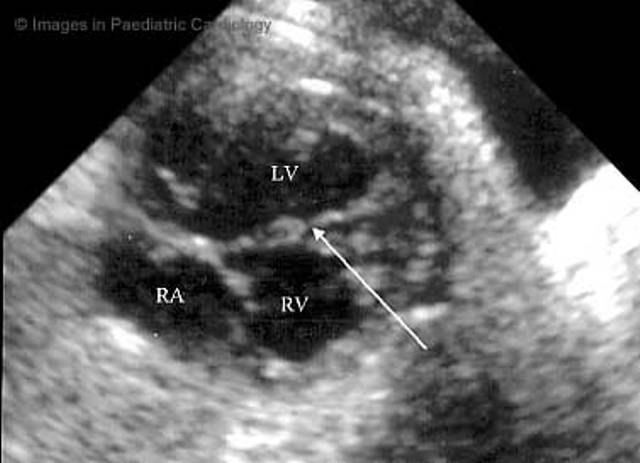
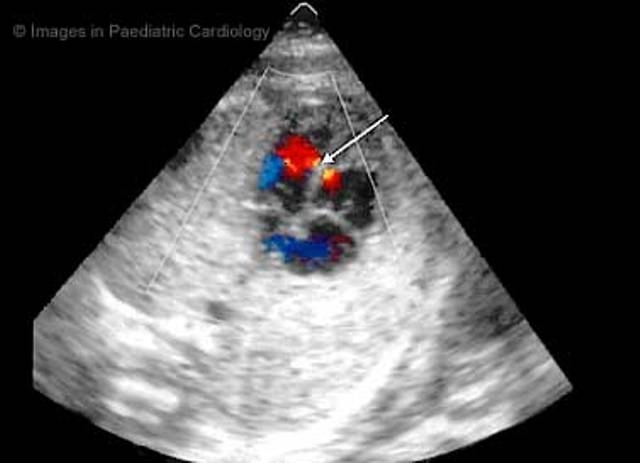
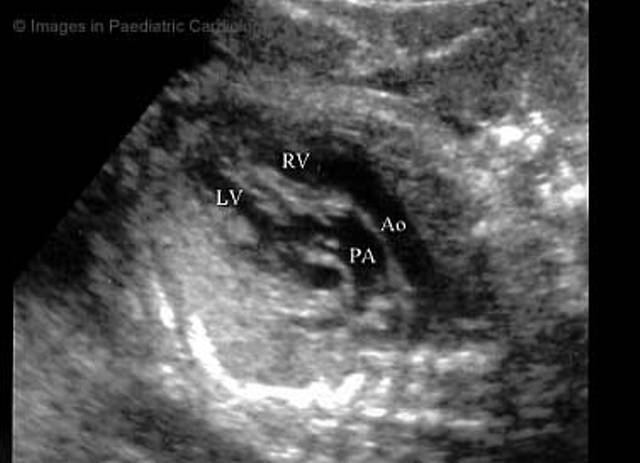
Keywords: congenital; fetal anomalies; fetal echocardiography; heart defects; prenatal diagnosis; ultrasonography.
Figures








References
-
- Steele MW, Breg WR. Chromosome analysis of human amniotic fluid cells. Lancet. 1966;1:383–385. - PubMed
-
- Chitayat D, Babul-Hirji R. Genetic counselling in prenatally diagnosed non-chromosomal fetal abnormalities. Curr Opin Obstet Gynecol. 2000;12:77–80. - PubMed
-
- Jenkins TM, Wapner RJ. First trimester prenatal diagnosis: chorionic villus sampling. Semin Perinatol. 1999;23:403–413. - PubMed
-
- Douglas Wilson R. Amniocentesis and chorionic villus sampling. Curr Opin Obstet Gynecol. 2000;12:81–86. - PubMed
-
- In: Fetal Abnormalities. Guidelines for Screeening, Diagnosis and Management. London, UK: RCPCH, RCOG; 1997. Royal College of Obstetricians and Gynaecologists, Royal College of Paediatrics and Child Health. Background evidence supporting the guidelines; p. 5.
LinkOut - more resources
Full Text Sources