

Balloon expandable stents for coarctation of the aorta: review of current status and technical considerations
- PMID: 22368626
- PMCID: PMC3232539
Item in Clipboard
Balloon expandable stents for coarctation of the aorta: review of current status and technical considerations
Images Paediatr Cardiol.
2003 Apr.
Abstract
Balloon expandable stents have been used to manage coarctation of the aorta in selected patients with very encouraging results. After the successful use of the Palmaz stents in these lesions newer stents as well as modifications of the Palmaz stents have been introduced to achieve optimal results in these patients. In this review, the older as well as the newer type stents used in coarctation are discussed. Technical considerations to achieve successful stent implantation and choice is outlined.
Keywords: catheter intervention; coarctation; congenital; heart disease; stent.
Figures
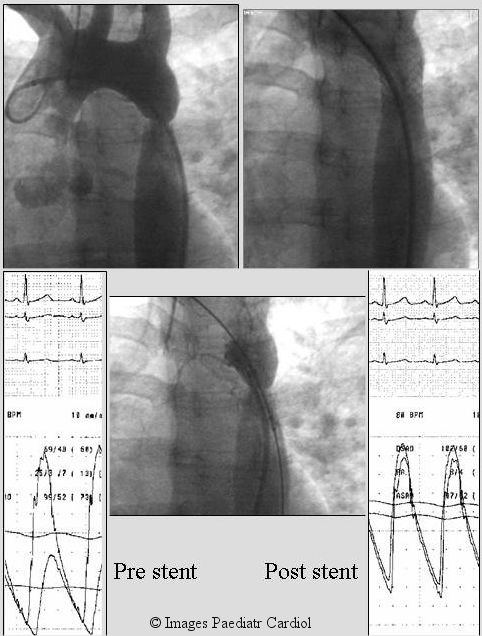
A 30 year old lady with poorly controlled hypertension was diagnosed to have native coarctation (A). A Palmaz P 308 stent was placed as a primary intervention. Post stent, there was no residual angiographic narrowing (B) or significant gradient. On follow-up her lower extremity blood pressure was higher than her arm pressure as is generally seen in normal individuals. She has been taken off anti hypertension treatment and remains normotensive.
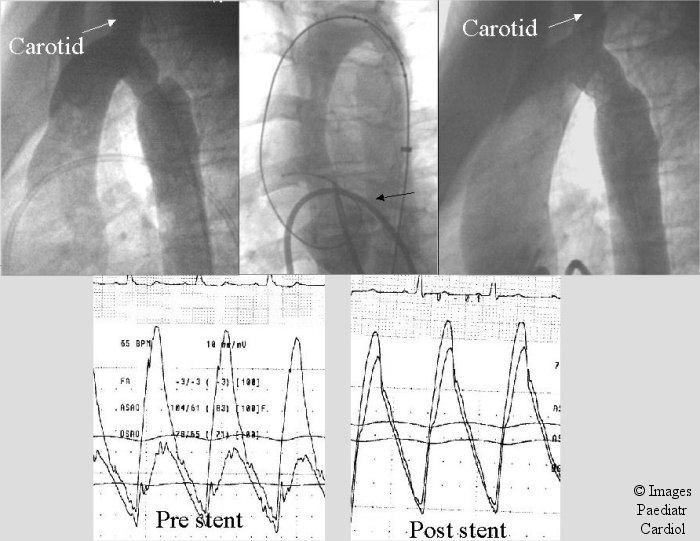
A 14 year old patient with recurrent coarctation after subclavian flap angioplasty. A transseptal approach (black arrow) was utilized to obtain accurate assessment of stent position prior to deployment to avoid the carotid artery. Notice accurate stent position in relation to the carotid. The systolic gradient decreased from 35 to 4 mm.Hg.
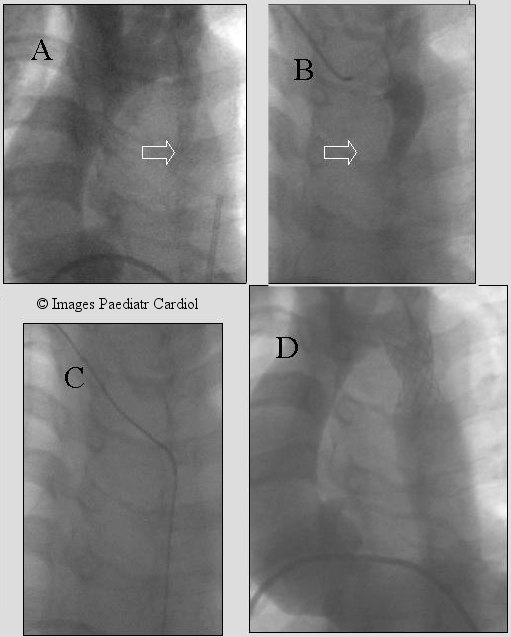
A 15 year old referred with diagnosis of coarctation (A & B) and poorly controlled hypertension. Angiogram shows severe coarctation seen better on lateral view (A). A Palmaz P-3110 stent (C & D) was placed eliminating the gradient which was 53 mm Hg.
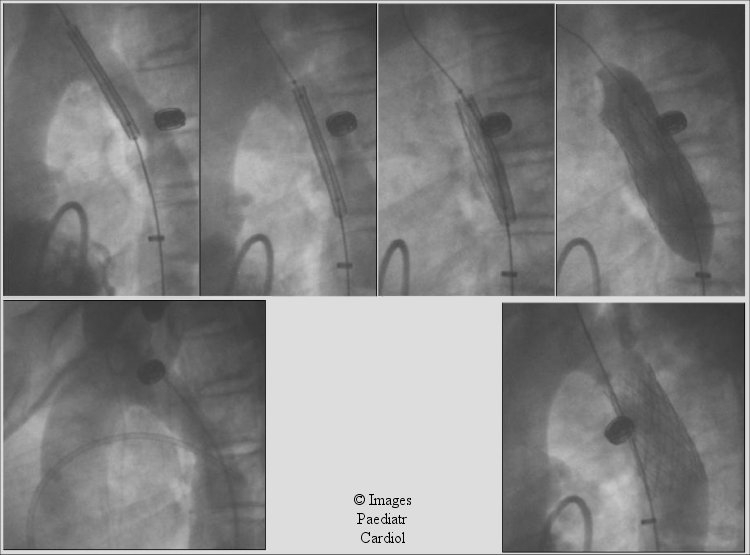
Recurrent coarctation involving a relatively long segment (A). A Palmaz P- 4010 stent was used (B). The wire was placed in the right subclavian (B-D). Notice the use of BIB balloon. Inflation of the inner balloon (D) allows for initial expansion of the stent center followed by the outer balloon (E). After implantation there was excellent angiographic and hemodynamic result (F).
Lateral projection of patient described in Figure 4. Notice the multiple angiograms obtained using the transseptally placed left ventricular catheter allowing for fine adjustment of stent position prior to deployment.
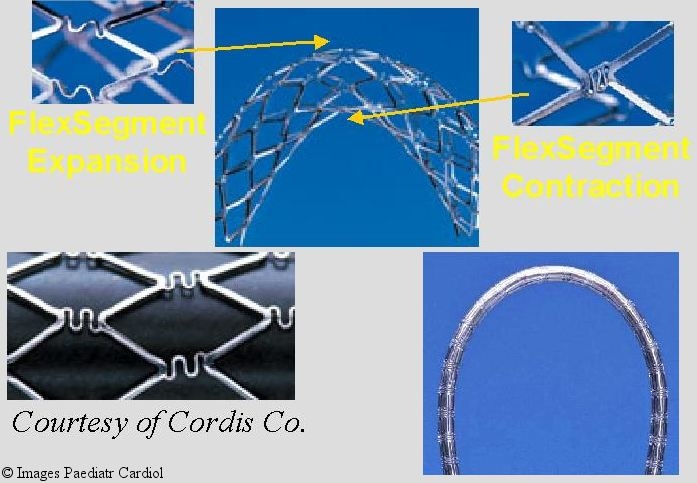
Flex segment technology used in manufacturing the Palmaz Genesis stent:allows for better negotiation of curves while maintaining radial strength
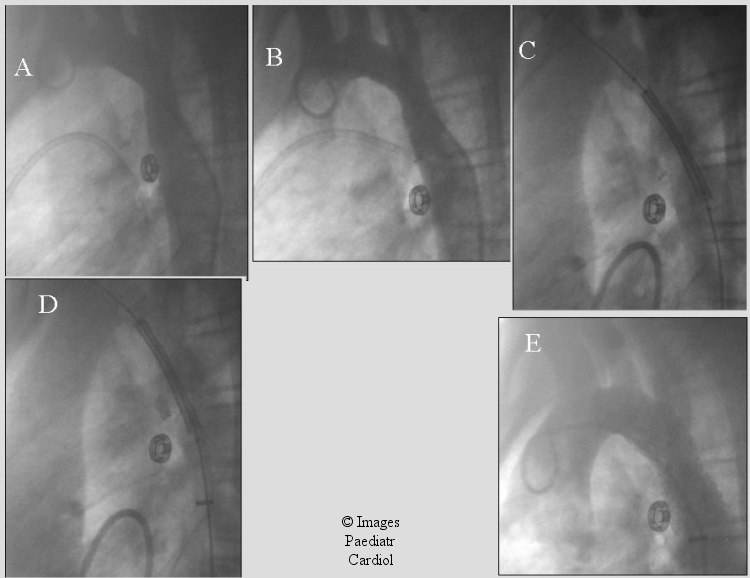
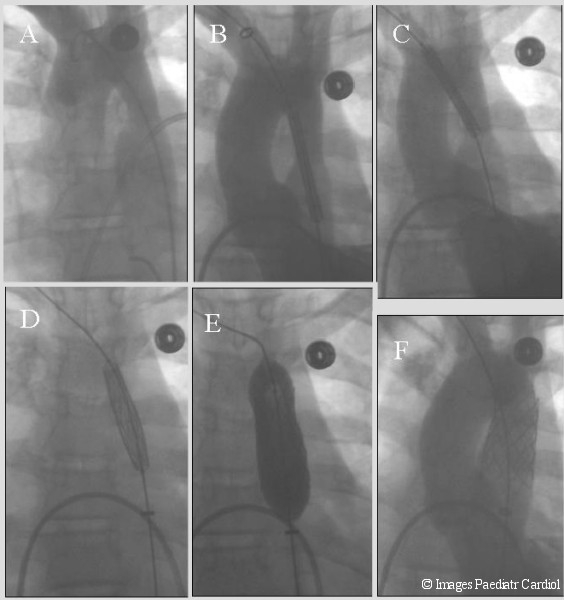
13 year old with recurrent coarctation after end to end repair. A) shows initial coarctation appearance. B) post balloon angioplasty there was mild improvement. Intra-therapeutics (Max) stent was subsequently placed (C & D). Stent position was adjusted based on the LV angiogram. E) The gradient decreased from 35 mm Hg to 1 mmHg after stent placement
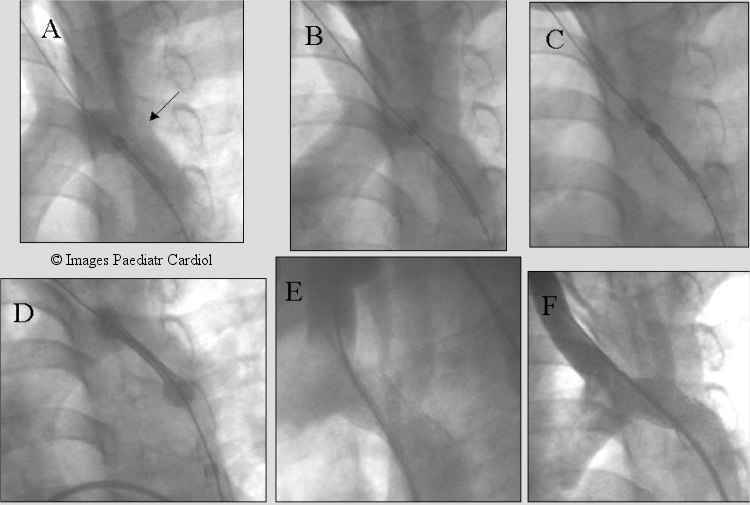
Recurrent coarctation after subclavian flap aortoplasty (arrow). Note the proximity to the left carotid artery. Multiple LV angiograms obtained to accurately place the stent before and after uncovering the stent. The two ends of the balloon were allowed to expand slightly (C & D) with further imaging prior to fully deploying the stent (Max, IT Stent).
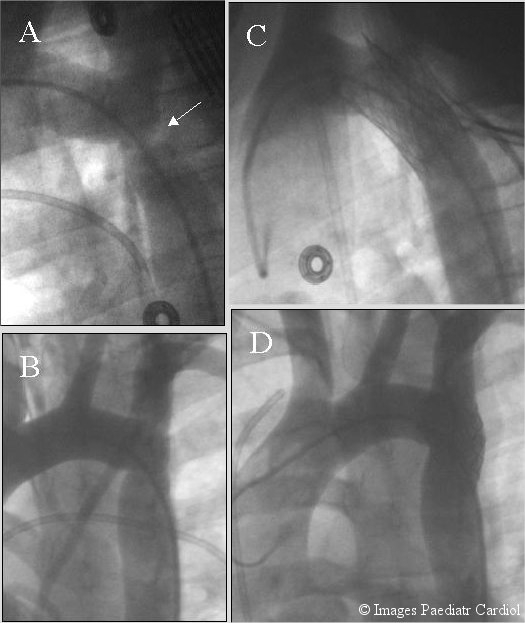
Severe native coarctation in a 12 year old. Retrograde crossing was difficult because of the presence of dilated collaterals. A wire was passed from the brachial artery (B & C), snared from the groin thus establishing the accurate track prior to successful stent placement (D). The gradient decreased at implantation from 80 mmHg to 25. Redilation was performed 9 months later.
References
-
- Anjos R, Quershi SA, Rosenthal E, Murdoch I, Hayes A, Parsons J, Baker EJ, Tynan M. Determinants of hemodynamic results of balloon dilation of aortic recoarctation. Am J Cardiol. 1992;69:665–671. - PubMed
-
- Kan JS, Whilte RI, Mitchell SE, Farmlett EJ, Donahoo JS, Gardner TJ. Treatment of restenosis of coarctation by percutaneous transluminal angioplasty. Circulation. 1983;68:1087–1094. - PubMed
-
- Lock JE, Keane JF, Fellows KE. The use of catheter intervention procedures for congenital heart disease. J Am Coll Cardiol. 1986;7:1420–1423. - PubMed
-
- Rao PS, Wilson AD, Chopra PS. Immediate and follow-up results of balloon angioplasty of postoperative recoarctation in infants and children. Am Heart J. 1990;120:1315–1320. - PubMed
-
- Rao PS. Balloon angioplasty of aortic coarctation: A review. Clin Cardiol. 1989;12:618–628. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources