

Lipoarabinomannan in urine during tuberculosis treatment: association with host and pathogen factors and mycobacteriuria
- PMID: 22369353
- PMCID: PMC3349560
- DOI: 10.1186/1471-2334-12-47
Lipoarabinomannan in urine during tuberculosis treatment: association with host and pathogen factors and mycobacteriuria
Abstract
Background: Detection of lipoarabinomannan (LAM), a Mycobacterium tuberculosis (Mtb) cell wall antigen, is a potentially attractive diagnostic. However, the LAM-ELISA assay has demonstrated variable sensitivity in diagnosing TB in diverse clinical populations. We therefore explored pathogen and host factors potentially impacting LAM detection.
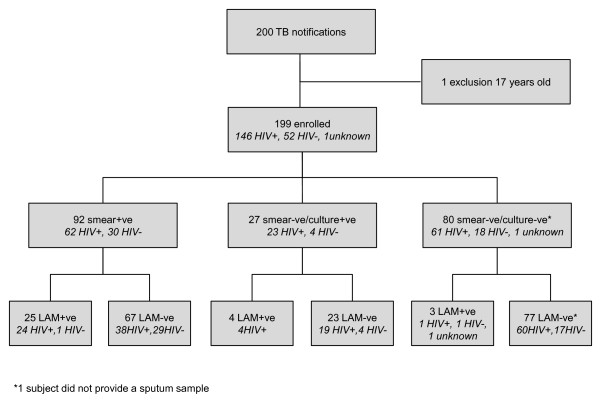
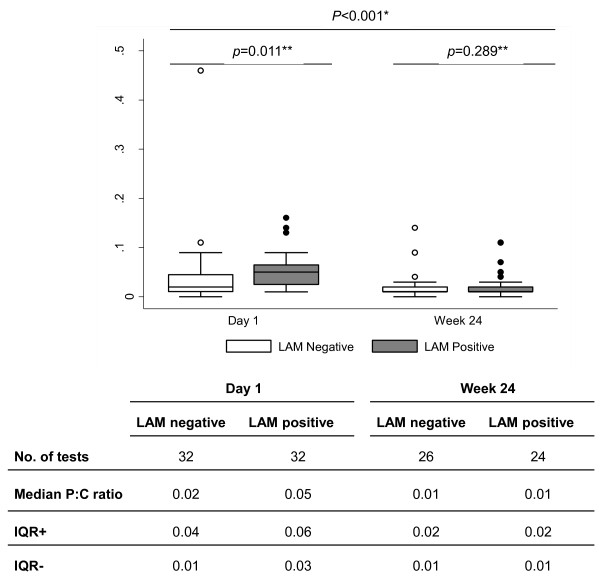
Methods: LAM-ELISA assay testing, sputum smear and culture status, HIV status, CD4 cell count, proteinuria and TB outcomes were prospectively determined in adults diagnosed with TB and commencing TB treatment at a South African township TB clinic. Sputum TB isolates were characterised by IS61110-based restriction fragment length polymorphism (RFLP) and urines were tested for mycobacteriuria by Xpert® MTB/RIF assay.
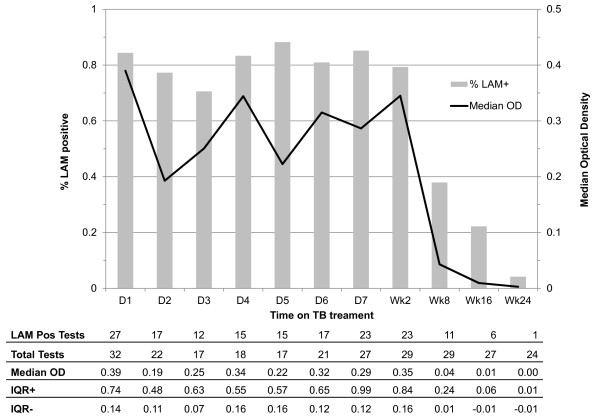
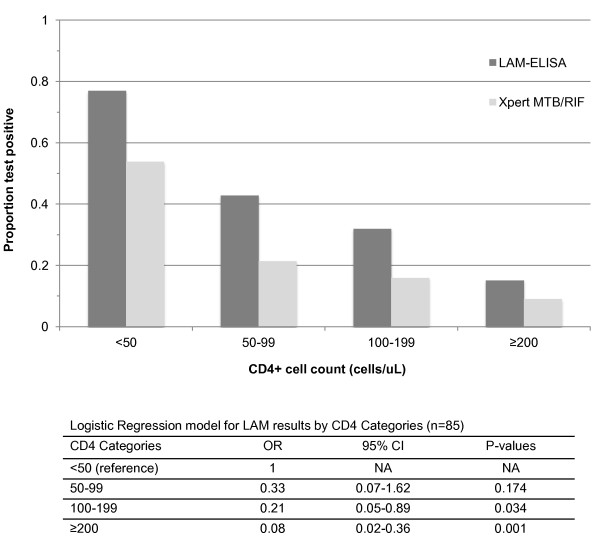
Results: 32/199 (16.1%) of patients tested LAM-ELISA positive. Median optical density and proportion testing LAM positive remained unchanged during 2 weeks of treatment and then declined over 24 weeks. LAM was associated with positive sputum smear and culture status, HIV infection and low CD4 cell counts but not proteinuria, RFLP strain or TB treatment outcome. The sensitivity of LAM for TB in HIV-infected patients with CD4 counts of ≥ 200, 100-199, 50-99, and < 50 cells/μl, was 15.2%, 32%, 42.9%, and 69.2% respectively. Mycobacteriuria was found in 15/32 (46.9%) of LAM positive patients and in none of the LAM negative controls.
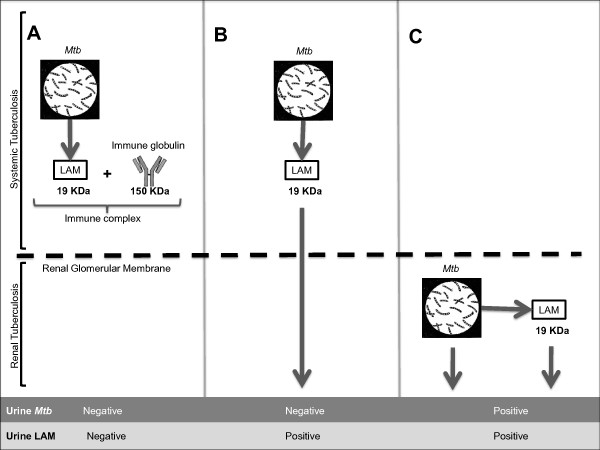
Conclusions: Urinary LAM was related to host immune factors, was unrelated to Mtb strain and declined steadily after an initial 2 weeks of TB treatment. The strong association of urine LAM with mycobacteriuria is a new finding, indicating frequent TB involvement of the renal tract in advanced HIV infection.
Figures
References
-
- Hunter SW, Gaylord H, Brennan PJ. Structure and antigenicity of the phosphorylated lipopolysaccharide antigens from the leprosy and tubercle bacilli. J Biol Chem. 1986;261(26):12345–12351. - PubMed
-
- Eleftheriadis T, Tsiaga P, Antoniadi G, Liakopoulos V, Kortsaris A, Giannatos E, Barbutis K, Stefanidis I, Vargemezis V. The value of serum antilipoarabinomannan antibody detection in the diagnosis of latent tuberculosis in hemodialysis patients. Am J Kidney Dis. 2005;46(4):706–712. doi: 10.1053/j.ajkd.2005.06.021. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
