

Tumor-specific fluorescence antibody imaging enables accurate staging laparoscopy in an orthotopic model of pancreatic cancer
- PMID: 22369743
- PMCID: PMC4096574
- DOI: 10.5754/hge11836
Tumor-specific fluorescence antibody imaging enables accurate staging laparoscopy in an orthotopic model of pancreatic cancer
Abstract
Background/aims: Laparoscopy is important in staging pancreatic cancer, but false negatives remain problematic. Making tumors fluorescent has the potential to improve the accuracy of staging laparoscopy.
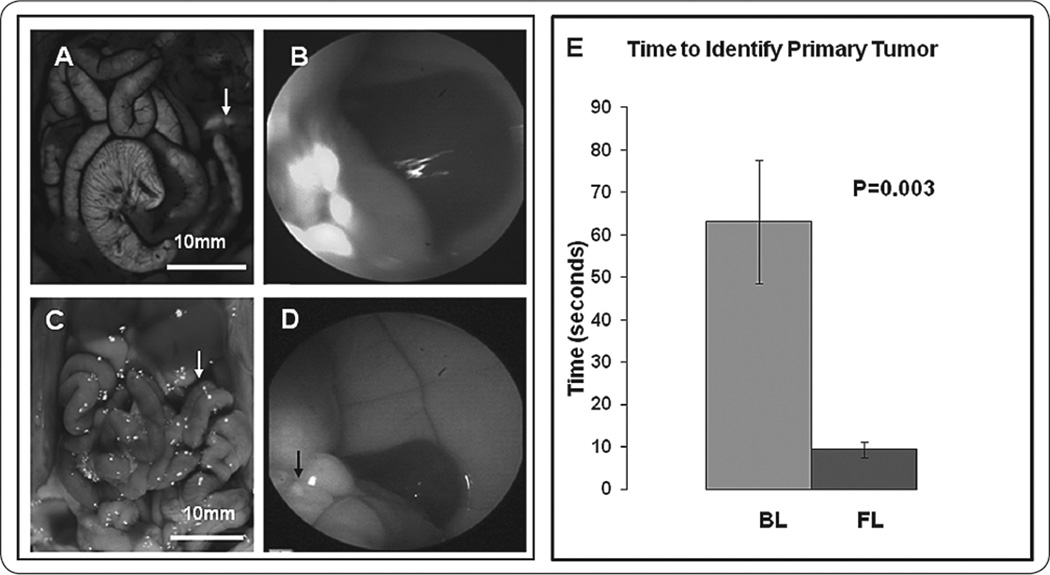
Methodology: Orthotopic and carcinomatosis models of pancreatic cancer were established with BxPC-3 human pancreatic cancer cells in nude mice. Alexa488-antiCEA conjugates were injected via tail vein 24 hours prior to laparoscopy. Mice were examined under bright field laparoscopic (BL) and fluorescence laparoscopic (FL) modes. Outcomes measured included time to identification of primary tumor for the orthotopic model and number of metastases identified within 2 minutes for the carcinomatosis model.
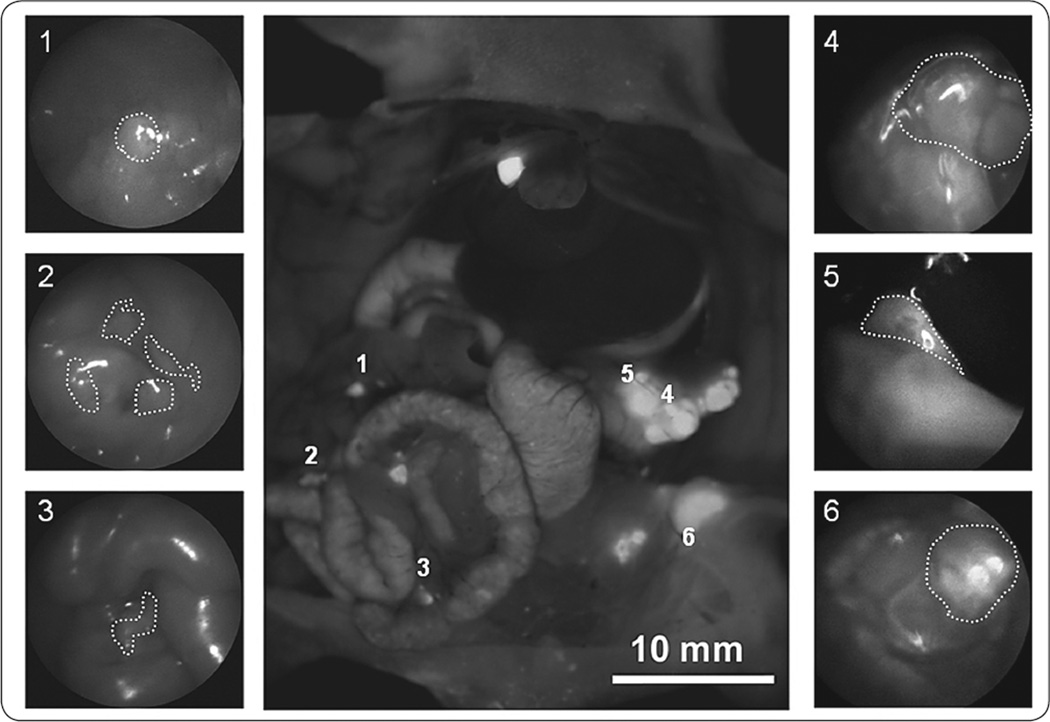
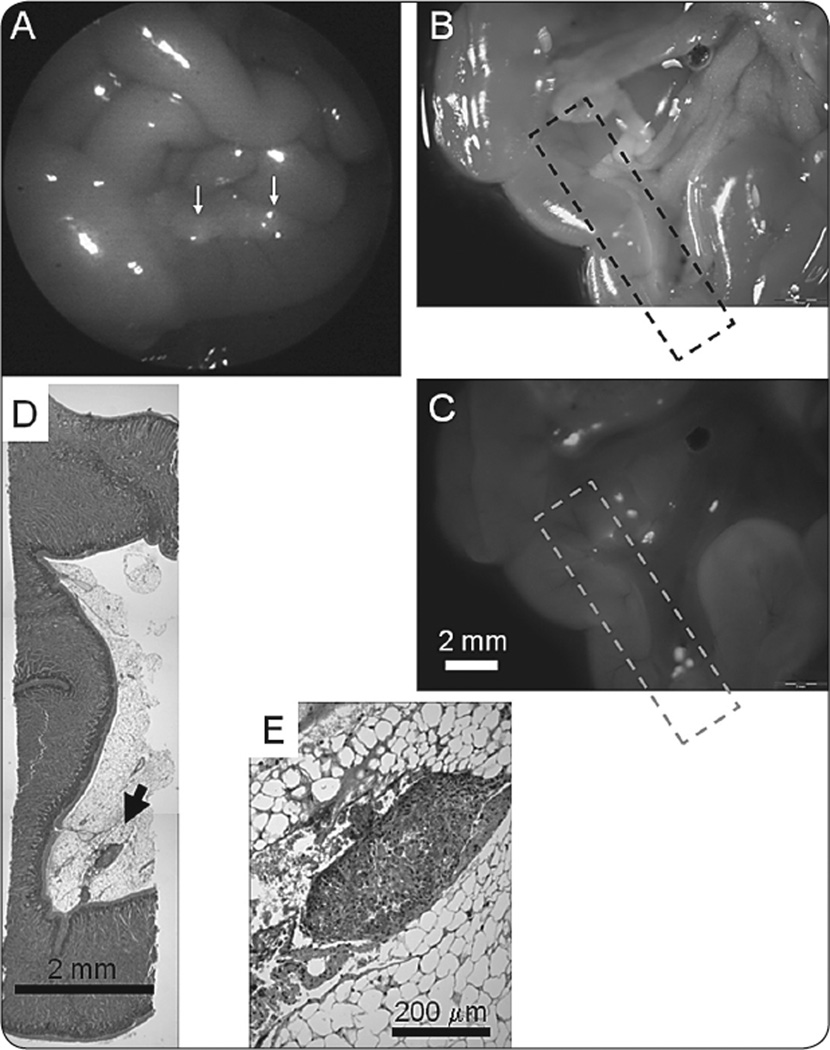
Results: FL enabled more rapid and accurate identification and localization of primary tumors and metastases than BL. Using BL took statistically significantly longer time than FL (p<0.0001, fold change and 95% CI for BL vs. FL: 8.12 (4.54,14.52)). More metastatic lesions were detected and localized under FL compared to BL and with greater accuracy, with sensitivities of 96% vs. 40%, respectively, when compared to control. FL was sensitive enough to detect metastatic lesions <1mm.
Conclusions: The use of fluorescence laparoscopy with tumors labeled with fluorophore-conjugated anti-CEA antibody permits rapid detection and accurate localization of primary and metastatic pancreatic cancer in an orthotopic model. The results of the present report demonstrate the future clinical potential of fluorescence laparoscopy.
Figures
Similar articles
-
Advantages of fluorescence-guided laparoscopic surgery of pancreatic cancer labeled with fluorescent anti-carcinoembryonic antigen antibodies in an orthotopic mouse model.J Am Coll Surg. 2014 Jul;219(1):132-41. doi: 10.1016/j.jamcollsurg.2014.02.021. Epub 2014 Mar 2. J Am Coll Surg. 2014. PMID: 24768506 Free PMC article.
-
Submillimeter-resolution fluorescence laparoscopy of pancreatic cancer in a carcinomatosis mouse model visualizes metastases not seen with standard laparoscopy.J Laparoendosc Adv Surg Tech A. 2011 Jul-Aug;21(6):485-9. doi: 10.1089/lap.2011.0181. Epub 2011 Jun 23. J Laparoendosc Adv Surg Tech A. 2011. PMID: 21699431 Free PMC article.
-
Tumor-Specific Labeling of Pancreatic Cancer Using a Humanized Anti-CEA Antibody Conjugated to a Near-Infrared Fluorophore.Ann Surg Oncol. 2018 Apr;25(4):1079-1085. doi: 10.1245/s10434-018-6344-6. Epub 2018 Jan 25. Ann Surg Oncol. 2018. PMID: 29372363 Free PMC article.
-
Toward Curative Fluorescence-Guided Surgery of Pancreatic Cancer.Hepatogastroenterology. 2015 May;62(139):715-22. Hepatogastroenterology. 2015. PMID: 26897960 Review.
-
Laparoscopy and peritoneal cytology in the staging of pancreatic cancer.J Hepatobiliary Pancreat Surg. 2000;7(1):15-20. doi: 10.1007/s005340050148. J Hepatobiliary Pancreat Surg. 2000. PMID: 10982586 Review.
Cited by
-
Fluorescence-guided surgery improves outcome in an orthotopic osteosarcoma nude-mouse model.J Orthop Res. 2014 Dec;32(12):1596-601. doi: 10.1002/jor.22706. Epub 2014 Aug 19. J Orthop Res. 2014. PMID: 25138581 Free PMC article.
-
Tumor-specific near-infrared nanobody probe rapidly labels tumors in an orthotopic mouse model of pancreatic cancer.Surgery. 2020 Jul;168(1):85-91. doi: 10.1016/j.surg.2020.02.020. Epub 2020 May 4. Surgery. 2020. PMID: 32370916 Free PMC article.
-
Intraoperative imaging-guided cancer surgery: from current fluorescence molecular imaging methods to future multi-modality imaging technology.Theranostics. 2014 Aug 15;4(11):1072-84. doi: 10.7150/thno.9899. eCollection 2014. Theranostics. 2014. PMID: 25250092 Free PMC article. Review.
-
Polyethylene glycol (PEG) linked to near infrared (NIR) dyes conjugated to chimeric anti-carcinoembryonic antigen (CEA) antibody enhances imaging of liver metastases in a nude-mouse model of human colon cancer.PLoS One. 2014 May 23;9(5):e97965. doi: 10.1371/journal.pone.0097965. eCollection 2014. PLoS One. 2014. PMID: 24859320 Free PMC article.
-
Specific tumor labeling enhanced by polyethylene glycol linkage of near infrared dyes conjugated to a chimeric anti-carcinoembryonic antigen antibody in a nude mouse model of human pancreatic cancer.J Biomed Opt. 2014;19(10):101504. doi: 10.1117/1.JBO.19.10.101504. J Biomed Opt. 2014. PMID: 24887695 Free PMC article.
References
-
- Jimenez RE, Warshaw AL, Rattner DW, et al. Impact of laparoscopic staging in the treatment of pancreatic cancer. Arch Surg. 2000;135:409–414. (discussion 414-405). - PubMed
-
- Verbeke CS. Resection margins and R1 rates in pancreatic cancer--are we there yet? Histopathology. 2008;52:787–796. - PubMed
-
- Kishimoto H, Kojima T, Watanabe Y, et al. In vivo imaging of lymph node metastasis with telomerase-specific replication-selective adenovirus. Nat Med. 2006;12:1213–1219. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical