

Topography, clinical, and genomic correlates of 5q myeloid malignancies revisited
- PMID: 22370328
- PMCID: PMC3341146
- DOI: 10.1200/JCO.2011.36.1824
Topography, clinical, and genomic correlates of 5q myeloid malignancies revisited
Abstract
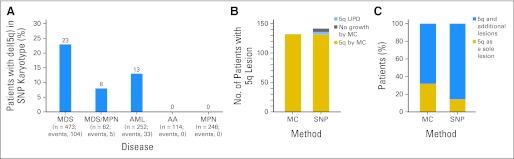
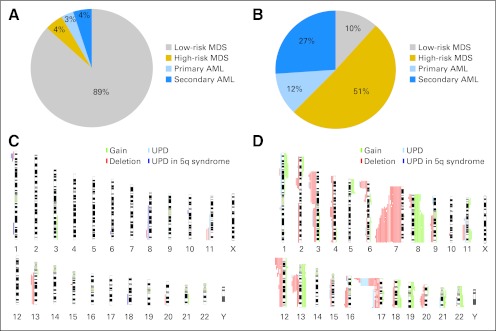
Purpose: Interstitial deletions of chromosome 5q are common in acute myeloid leukemia (AML) and myelodysplastic syndromes (MDS), pointing toward the pathogenic role of this region in disease phenotype and clonal evolution. The higher level of resolution of single-nucleotide polymorphism array (SNP-A) karyotyping may be used to find cryptic abnormalities and to precisely define the topographic features of the genomic lesions, allowing for more accurate clinical correlations.
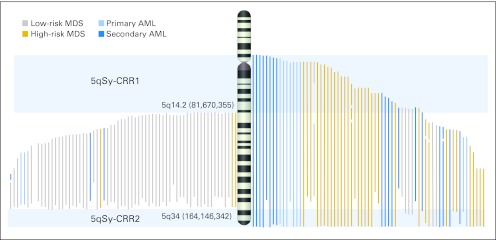
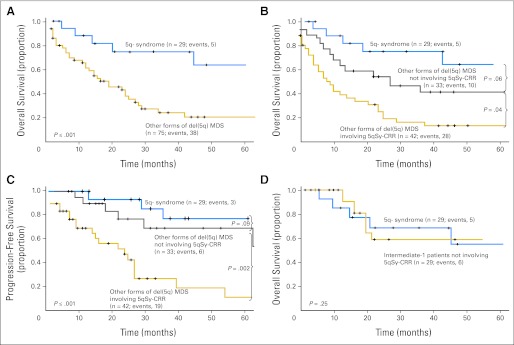
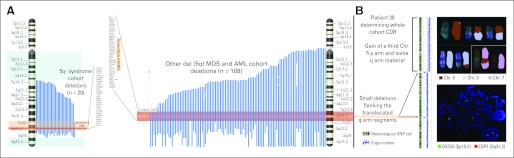
Patients and methods: We analyzed high-density SNP-A karyotyping at diagnosis for a cohort of 1,155 clinically well-annotated patients with malignant myeloid disorders. results: We identified chromosome 5q deletions in 142 (12%) of 1,155 patients and uniparental disomy segments (UPD) in four (0.35%) of 1,155 patients. Patients with deletions involving the centromeric and telomeric extremes of 5q have a more aggressive disease phenotype and additional chromosomal lesions. Lesions not involving the centromeric or telomeric extremes of 5q are not exclusive to 5q- syndrome but can be associated with other less aggressive forms of MDS. In addition, larger 5q deletions are associated with either del(17p) or UPD17p. In 31 of 33 patients with del(5q) AML, either a deletion involving the centromeric and/or telomeric regions or heterozygous mutations in NPM1 or MAML1 located in 5q35 were present.
Conclusion: Our results suggest that the extent of the affected region on 5q determines clinical characteristics that can be further modified by heterozygous mutations present in the telomeric extreme.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Solé F, Espinet B, Sanz GF, et al. Incidence, characterization and prognostic significance of chromosomal abnormalities in 640 patients with primary myelodysplastic syndromes: Grupo Cooperativo Espanol de Citogenetica Hematologica. Br J Haematol. 2000;108:346–356. - PubMed
-
- Tefferi A, Vardiman JW. Myelodysplastic syndromes. N Engl J Med. 2009;361:1872–1885. - PubMed
-
- Nimer SD. Clinical management of myelodysplastic syndromes with interstitial deletion of chromosome 5q. J Clin Oncol. 2006;24:2576–2582. - PubMed
-
- Grimwade D, Walker H, Oliver F, et al. The importance of diagnostic cytogenetics on outcome in AML: Analysis of 1,612 patients entered into the MRC AML 10 trial—The Medical Research Council Adult and Children's Leukaemia Working Parties. Blood. 1998;92:2322–2333. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
