

Understanding fragmentation of prostate cancer survivorship care: implications for cost and quality
- PMID: 22370955
- PMCID: PMC4860006
- DOI: 10.1002/cncr.26601
Understanding fragmentation of prostate cancer survivorship care: implications for cost and quality
Abstract
Background: Cancer survivors are particularly prone to the effects of a fragmented health care delivery system. The implications of fragmented cancer care across providers likely include greater spending and worse quality of care. For this reason, the authors measured relations between increasing fragmentation of cancer care, expenditures, and quality of care among prostate cancer survivors.
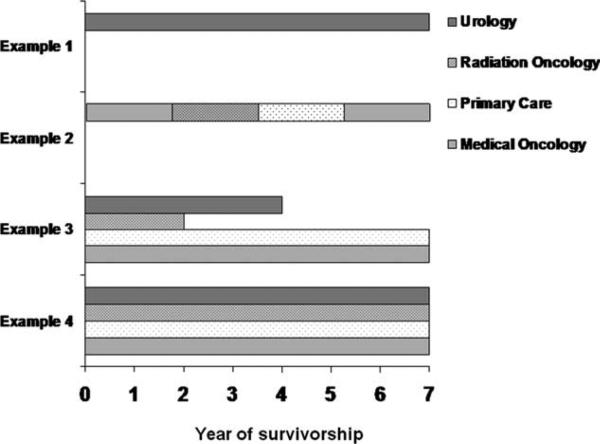
Methods: A total of 67,736 patients diagnosed with prostate cancer between 1992 and 2005 were identified using Surveillance, Epidemiology, and End Results (SEER)-Medicare data. Using the Herfindahl-Hirschman Index and a measure of the average number of prostate cancer providers over time, patients were sorted into 3 fragmentation groups (low, intermediate, and high). The authors then examined annual per capita survivorship expenditures and a measure of quality (ie, repetitive prostate-specific antigen [PSA] testing within 30 days) according to their fragmentation exposure using multinomial logistic regression.
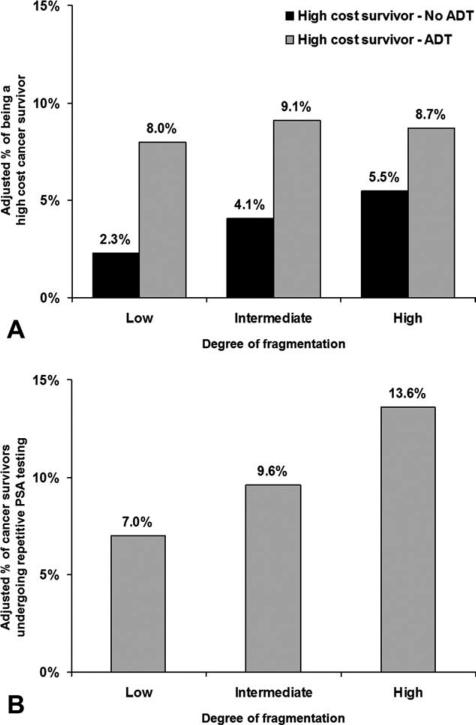
Results: Patients with highly fragmented cancer care tended to be younger, white, and of higher socioeconomic status (all P < .001). Prostate cancer survivorship interventions were most common among patients with the highest fragmentation of care across providers (P < .001). After adjustment for clinical characteristics and prostate cancer survivorship interventions, higher degrees of fragmentation continued to be associated with repetitive PSA testing (13.6% for high vs 7.0% for low fragmentation; P < .001) and greater spending, particularly among patients not treated with androgen deprivation therapy.
Conclusions: Fragmented prostate cancer survivorship care is expensive and associated with potentially unnecessary services. Efforts to improve care coordination via current policy initiatives, electronic medical records, and the implementation of cancer survivorship tools may help to decrease fragmentation of care and mitigate downstream consequences for prostate cancer survivors.
Copyright © 2011 American Cancer Society.
Figures
Similar articles
-
The economic burden of prostate cancer survivorship care.J Urol. 2010 Aug;184(2):532-8. doi: 10.1016/j.juro.2010.03.136. Epub 2010 Jun 17. J Urol. 2010. PMID: 20620413
-
Caring for Alaska Native prostate cancer survivors in primary care: a survey of Alaska Tribal Health System providers.Int J Circumpolar Health. 2014 Feb 27;73:23637. doi: 10.3402/ijch.v73.23637. eCollection 2014. Int J Circumpolar Health. 2014. PMID: 24596707 Free PMC article.
-
Primary care perspectives on prostate cancer survivorship: implications for improving quality of care.Urol Oncol. 2013 Aug;31(6):727-32. doi: 10.1016/j.urolonc.2011.06.002. Epub 2011 Jul 20. Urol Oncol. 2013. PMID: 21775171 Free PMC article.
-
Providing prostate cancer survivorship care in Japan: Implications from the USA care model.Int J Urol. 2016 Nov;23(11):906-915. doi: 10.1111/iju.13186. Epub 2016 Sep 13. Int J Urol. 2016. PMID: 27624609 Review.
-
Shifting focus to cancer survivorship in prostate cancer: challenges and opportunities.Curr Opin Urol. 2008 May;18(3):326-32. doi: 10.1097/MOU.0b013e3282f9b3ff. Curr Opin Urol. 2008. PMID: 18382244 Review.
Cited by
-
Patterns and Impact of Fragmented Care in Stage II and III Gastric Cancer.Ann Surg Oncol. 2022 Sep;29(9):5422-5431. doi: 10.1245/s10434-022-12031-z. Epub 2022 Jun 20. Ann Surg Oncol. 2022. PMID: 35723791 Free PMC article.
-
Health policy: lost in transition, losing money, but caution precludes a "quick fix".Nat Rev Urol. 2011 Dec 13;9(1):14-6. doi: 10.1038/nrurol.2011.205. Nat Rev Urol. 2011. PMID: 22158595 Free PMC article.
-
Prostate Cancer Surveillance After Radiation Therapy in a National Delivery System.Fed Pract. 2019 Feb;36(Suppl 1):S16-S21. Fed Pract. 2019. PMID: 30867631 Free PMC article.
-
Patient and Healthcare Provider Perspectives on the Implementation of a Web-Based Clinical Communication System for Cancer: A Qualitative Study.Curr Oncol. 2022 Nov 3;29(11):8401-8414. doi: 10.3390/curroncol29110662. Curr Oncol. 2022. PMID: 36354722 Free PMC article.
-
Continuity of Care, Follow-Up Care, and Outcomes among Breast Cancer Survivors.Int J Environ Res Public Health. 2019 Aug 22;16(17):3050. doi: 10.3390/ijerph16173050. Int J Environ Res Public Health. 2019. PMID: 31443512 Free PMC article.
References
-
- Enthoven AC. Integrated delivery systems: the cure for fragmentation. Am J Manag Care. 2009;15(suppl 10):S284–S290. - PubMed
-
- Shih A, Davis K, Schoenbaum S, et al. Organizing the U.S. Health Care Delivery System for High Performance. The Commonwealth Fund. 2008 Aug;
-
- McCarthy D, Nuzum R, Mika S, et al. The North Dakota Experience: Achieving High-Performance Health Care Through Rural Innovation and Cooperation. The Commonwealth Fund. 2008 May;
-
- Schrag D, Xu F, Hanger M, Elkin E, Bickell NA, Bach PB. Fragmentation of care for frequently hospitalized urban residents. Med Care. 2006;44:560–567. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
