

Cliniconeuropathologic correlations show astroglial albumin storage as a common factor in epileptogenic vascular lesions
- PMID: 22372630
- PMCID: PMC3669690
- DOI: 10.1111/j.1528-1167.2012.03405.x
Cliniconeuropathologic correlations show astroglial albumin storage as a common factor in epileptogenic vascular lesions
Abstract
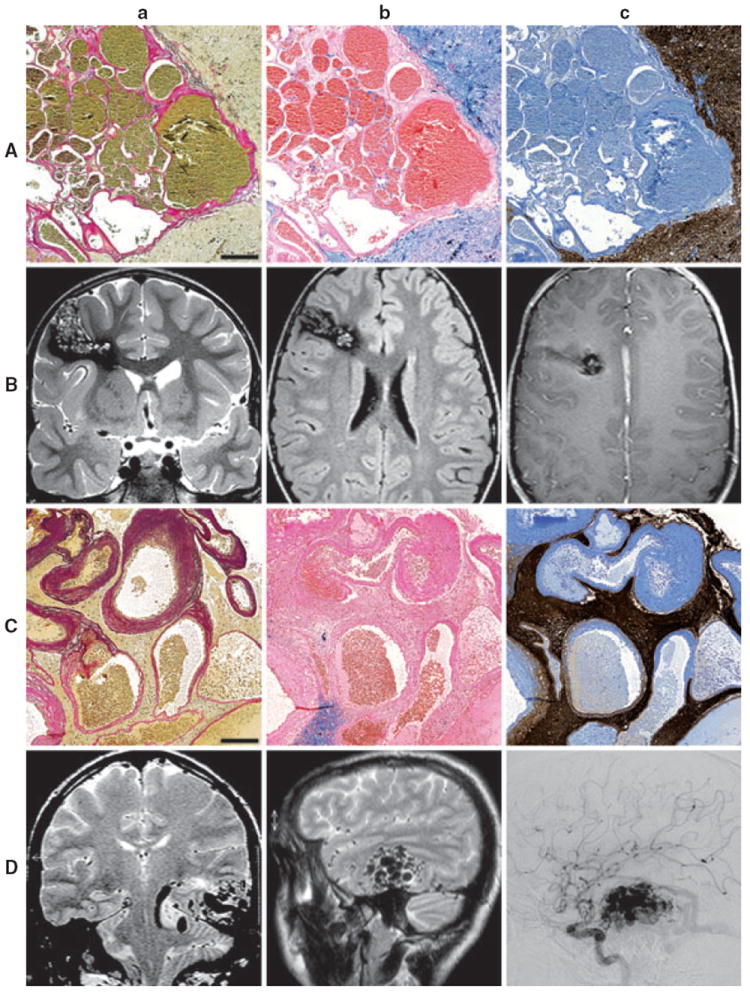
Purpose: Intracerebral vascular malformations including cavernous angiomas (CAs) and arteriovenous malformations (AVMs) are an important cause of chronic pharmacoresistant epilepsies. Little is known about the pathogenetic basis of epilepsy in patients with vascular malformations. Intracerebral deposits of iron-containing blood products have been generally regarded as responsible for the strong epileptogenic potential of CAs. Here, we have analyzed whether blood-brain barrier (BBB) dysfunction and subsequent astrocytic albumin uptake, recently described as critical trigger of focal epilepsy, represent pathogenetic factors in vascular lesion-associated epileptogenesis.
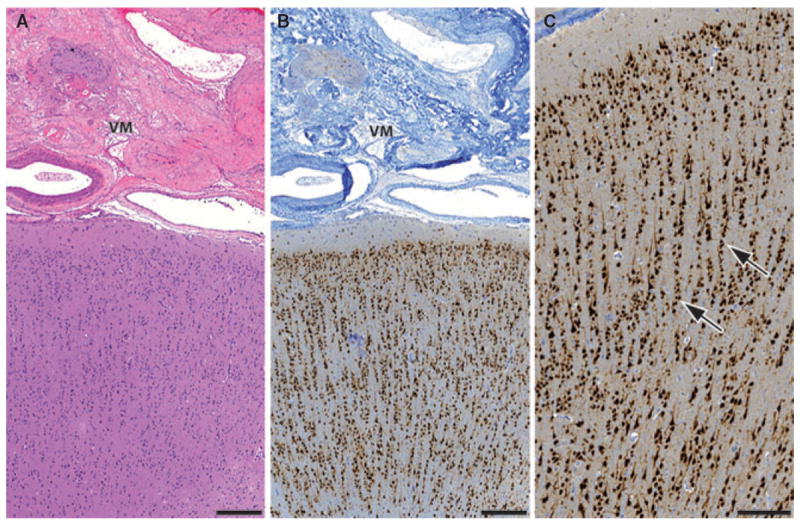
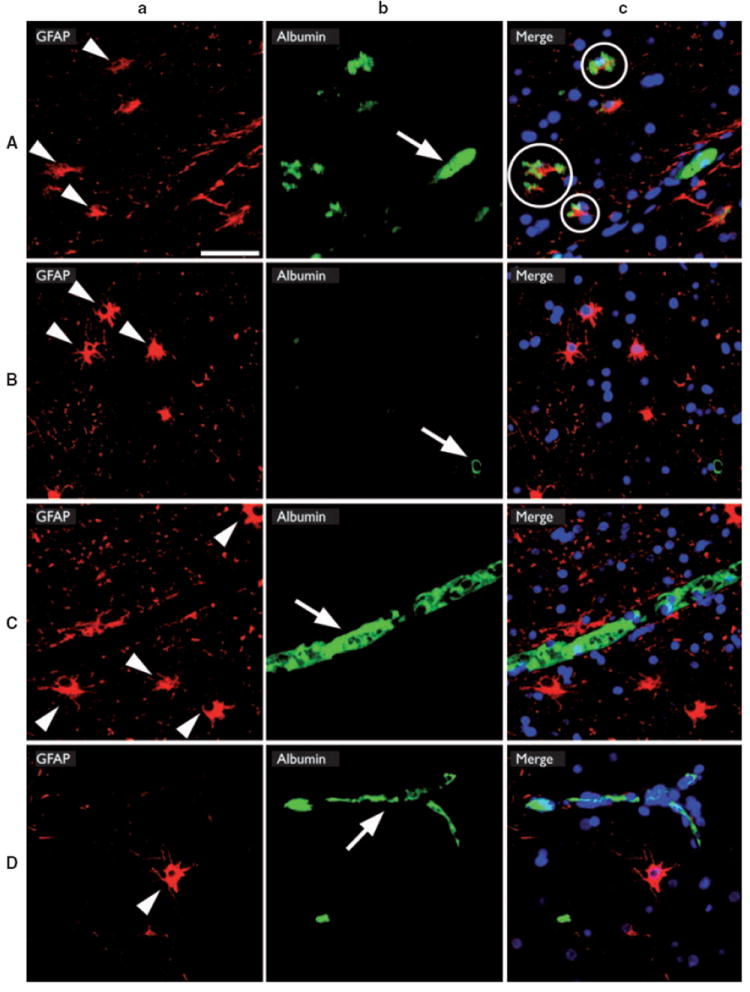
Methods: We examined the correlation between hemosiderin deposits, albumin accumulation, and several clinical characteristics in a series of 80 drug-refractory epilepsy patients with CAs or AVMs who underwent surgical resection. Analysis of clinical parameters included gender, age of seizure onset, epilepsy frequency, duration of epilepsy before surgery, and postoperative seizure outcome classification according to Engel class scale. Hemosiderin deposits in the adjacent brain tissue of the vascular lesion were semiquantitatively analyzed. Fluorescent double-immunohistochemistry using GFAP/albumin costaining was performed to study albumin extravasation.
Key findings: Our results suggest that a shorter duration of preoperative epilepsy is correlated with significantly better postsurgical outcome (p < 0.05), whereas no additional clinical or neuropathologic parameter correlated significantly with the postsurgical seizure situation. Intriguingly, we observed strong albumin immunoreactivity within the vascular lesion and in perilesional astrocytes (57.65 ± 4.05%), but not in different control groups.
Significance: Our present data on albumin uptake in brain tissue adjacent to AVMs and CAs suggests BBB dysfunction and accumulation of albumin within astrocytes as a new pathologic feature potentially associated with the epileptogenic mechanism for vascular lesions and provides novel therapy perspectives for antiepileptogenesis in affected patients.
Wiley Periodicals, Inc. © 2012 International League Against Epilepsy.
Conflict of interest statement
None of the authors has any conflict of interest to disclose. We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Figures

References
-
- Awad I, Jabbour P. Cerebral cavernous malformations and epilepsy. Neurosurg Focus. 2006;21:e7. - PubMed
-
- Ballabh P, Braun A, Nedergaard M. The blood–brain barrier: an overview: structure, regulation, and clinical implications. Neurobiol Dis. 2004;16:1–13. - PubMed
-
- Baumann CR, Schuknecht B, Lo Russo G, Cossu M, Citterio A, Andermann F, Siegel AM. Seizure outcome after resection of cavernous malformations is better when surrounding hemosiderin-stained brain also is removed. Epilepsia. 2006;47:563–566. - PubMed
-
- Baumann CR, Acciarri N, Bertalanffy H, Devinsky O, Elger CE, Lo Russo G, Cossu M, Sure U, Singh A, Stefan H, Hammen T, Georgiadis D, Baumgartner RW, Andermann F, Siegel AM. Seizure outcome after resection of supratentorial cavernous malformations: a study of 168 patients. Epilepsia. 2007;48:559–563. - PubMed
-
- Blumcke I, Thom M, Aronica E, Armstrong DD, Vinters HV, Palmini A, Jacques TS, Avanzini G, Barkovich AJ, Battaglia G, Becker A, Cepeda C, Cendes F, Colombo N, Crino P, Cross JH, Delalande O, Dubeau F, Duncan J, Guerrini R, Kahane P, Mathern G, Najm I, Ozkara C, Raybaud C, Represa A, Roper SN, Salamon N, Schulze-Bonhage A, Tassi L, Vezzani A, Spreafico R. The clinicopathologic spectrum of focal cortical dysplasias: a consensus classification proposed by an ad hoc Task Force of the ILAE Diagnostic Methods Commission. Epilepsia. 2011;52:158–174. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
