

Preoperative characteristics of high-Gleason disease predictive of favourable pathological and clinical outcomes at radical prostatectomy
- PMID: 22373045
- PMCID: PMC4124597
- DOI: 10.1111/j.1464-410X.2012.10986.x
Preoperative characteristics of high-Gleason disease predictive of favourable pathological and clinical outcomes at radical prostatectomy
Abstract
What's known on the subject? and What does the study add? Men with high-risk prostate cancer experience recurrence, metastases and death at the highest rate in the prostate cancer population. Pathological stage at radical prostatectomy (RP) is the greatest predictor of recurrence and mortality in men with high-grade disease. Preoperative models predicting outcome after RP are skewed by the large proportion of men with low- and intermediate-risk features; there is a paucity of data about preoperative criteria to identify men with high-grade cancer who may benefit from RP. The present study adds comprehensive biopsy data from a large cohort of men with high-grade prostate cancer at biopsy. By adding biopsy parameters, e.g. number of high-grade cores and >50% involvement of any core, to traditional predictors of outcome (prostate-specific antigen concentration, clinical stage and Gleason sum), we can better inform men who present with high-grade prostate cancer as to their risk of favourable or unfavourable disease at RP.
Objective: To investigate preoperative characteristics that distinguish favourable and unfavourable pathological and clinical outcomes in men with high biopsy Gleason sum (8-10) prostate cancer to better select men who will most benefit from radical prostatectomy (RP).
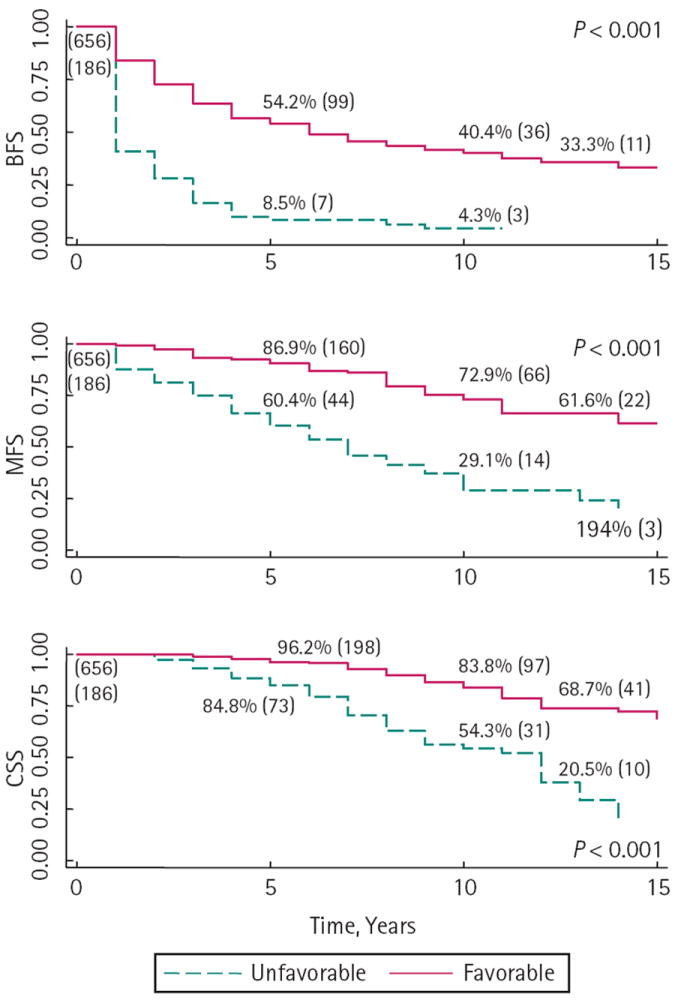
Patients and methods: The Institutional Review Board-approved institutional RP database (1982-2010) was analysed for men with high-Gleason prostate cancer on biopsy; 842 men were identified. The 10-year biochemical-free (BFS), metastasis-free (MFS) and prostate cancer-specific survival (CSS) were calculated using the Kaplan-Meier method to verify favourable pathology as men with Gleason <8 at RP or ≤ pT3a compared with men with unfavourable pathology with Gleason 8-10 and pT3b or N1. Preoperative characteristics were compared using appropriate comparative tests. Logistic regression determined preoperative predictors of unfavourable pathology.
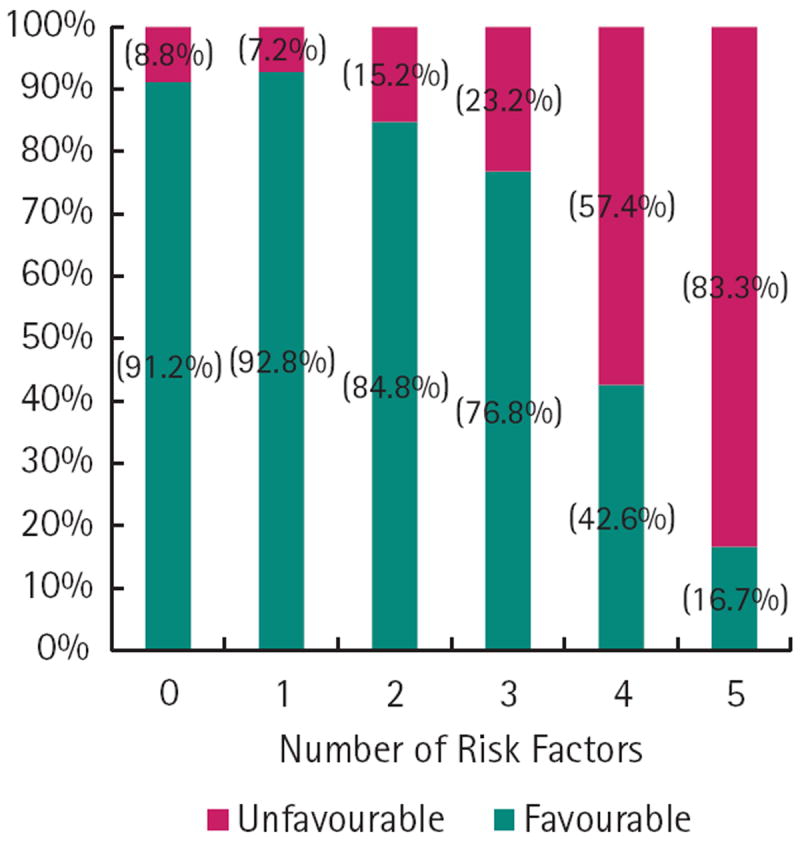
Results: There was favourable pathology in 656 (77.9%) men. The 10-year BFS, MFS and CSS were 31.0%, 60.9% and 74.8%, respectively. In contrast, men with unfavourable pathological findings had significantly worse 10-year BFS, MFS and CSS, at 4.3%, 29.1% and 52.3%, respectively (all P < 0.001). In multivariable logistic regression, a prostate-specific antigen (PSA) concentration of >10 ng/mL (odds ratio [OR] 2.24, 95% confidence interval [CI] 1.38-3.62, P = 0.001), advanced clinical stage (≥ cT2b; OR 2.55, 95% CI 1.55-4.21, P < 0.001), Gleason pattern 9 or 10 at biopsy (OR 2.55, 95% CI 1.59-4.09, P < 0.001), increasing number of cores positive with high-grade cancer (OR 1.16, 95% CI 1.01-1.34, P = 0.04) and >50% positive core involvement (OR 2.25, 95% CI 1.17-4.35, P = 0.015) were predictive of unfavourable pathology.
Conclusions: Men with high-Gleason sum at biopsy are at high risk for biochemical recurrence, metastasis and death after RP; men with high Gleason sum and advanced pathological stage (pT3b or N1) have the worst prognosis. Among men with high-Gleason sum at biopsy, a PSA concentration of >10 ng/mL, clinical stage ≥ T2b, Gleason pattern 9 or 10, increasing number of cores with high-grade cancer and >50% core involvement are predictive of unfavourable pathology.
© 2012 THE AUTHORS. BJU INTERNATIONAL © 2012 BJU INTERNATIONAL.
Conflict of interest statement
None declared.
Figures
References
-
- Grossfeld GD, Latini DM, Lubeck DP, Mehta SS, Carroll PR. Predicting recurrence after radical prostatectomy for patients with high risk prostate cancer. J Urol. 2003;169:157–63. - PubMed
-
- Pound CR, Partin AW, Epstein JI, Walsh PC. Prostate-specific antigen after anatomic radical retropubic prostatectomy. Patterns of recurrence and cancer control. Urol Clin North Am. 1997;24:395–406. - PubMed
-
- D’Amico AV, Whittington R, Malkowicz SB, et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA. 1998;280:969–74. - PubMed
-
- Han M, Partin AW, Pound CR, Epstein JI, Walsh PC. Long-term biochemical disease-free and cancer-specific survival following anatomic radical retropubic prostatectomy. The 15-year Johns Hopkins experience. Urol Clin North Am. 2001;28:555–65. - PubMed
-
- Partin AW, Yoo J, Carter HB, et al. The use of prostate specific antigen, clinical stage and Gleason score to predict pathological stage in men with localized prostate cancer. Journal Urol. 1993;150:110–4. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
