

Association of body temperature and antipyretic treatments with mortality of critically ill patients with and without sepsis: multi-centered prospective observational study
- PMID: 22373120
- PMCID: PMC3396278
- DOI: 10.1186/cc11211
Association of body temperature and antipyretic treatments with mortality of critically ill patients with and without sepsis: multi-centered prospective observational study
Erratum in
- Crit Care. 2012;16(1):450
Abstract
Introduction: Fever is frequently observed in critically ill patients. An independent association of fever with increased mortality has been observed in non-neurological critically ill patients with mixed febrile etiology. The association of fever and antipyretics with mortality, however, may be different between infective and non-infective illness.
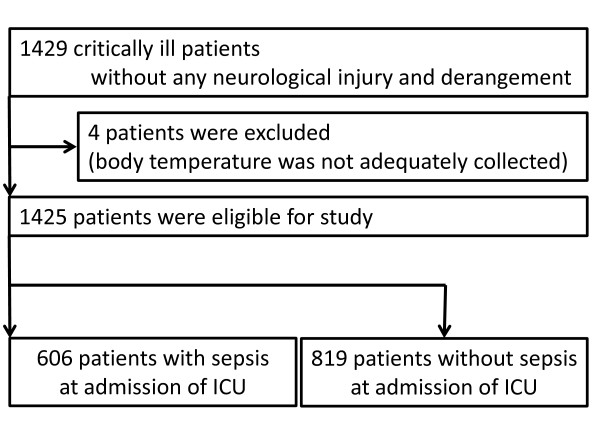
Methods: We designed a prospective observational study to investigate the independent association of fever and the use of antipyretic treatments with mortality in critically ill patients with and without sepsis. We included 1,425 consecutive adult critically ill patients (without neurological injury) requiring >48 hours intensive care admitted in 25 ICUs. We recorded four-hourly body temperature and all antipyretic treatments until ICU discharge or 28 days after ICU admission, whichever occurred first. For septic and non-septic patients, we separately assessed the association of maximum body temperature during ICU stay (MAXICU) and the use of antipyretic treatments with 28-day mortality.
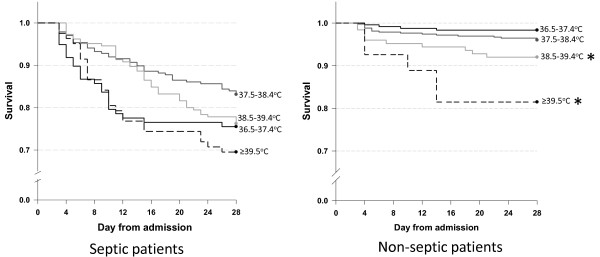
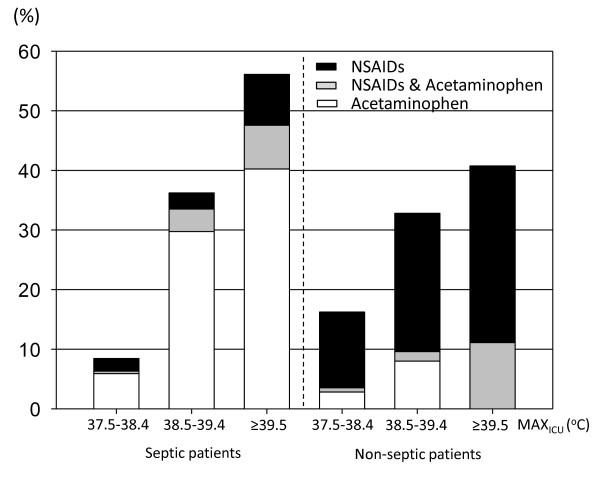
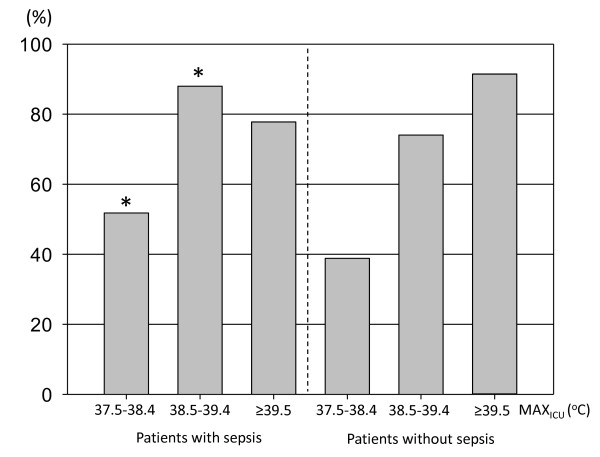
Results: We recorded body temperature 63,441 times. Antipyretic treatment was given 4,863 times to 737 patients (51.7%). We found that treatment with non-steroidal anti-inflammatory drugs (NSAIDs) or acetaminophen independently increased 28-day mortality for septic patients (adjusted odds ratio: NSAIDs: 2.61, P=0.028, acetaminophen: 2.05, P=0.01), but not for non-septic patients (adjusted odds ratio: NSAIDs: 0.22, P=0.15, acetaminophen: 0.58, P=0.63). Application of physical cooling did not associate with mortality in either group. Relative to the reference range (MAXICU ≥ 39.5°C increased risk of 28-day mortality in non-septic patients (adjusted odds ratio 8.14, P=0.01), but not in septic patients (adjusted odds ratio 0.47, P=0.11) [corrected].
Conclusions: In non-septic patients, high fever (≥39.5°C) independently associated with mortality, without association of administration of NSAIDs or acetaminophen with mortality. In contrast, in septic patients, administration of NSAIDs or acetaminophen independently associated with 28-day mortality, without association of fever with mortality. These findings suggest that fever and antipyretics may have different biological or clinical or both implications for patients with and without sepsis.
Trial registration: ClinicalTrials.gov: NCT00940654.
Figures
Comment in
-
Good and bad fever.Crit Care. 2012 Dec 12;16(2):119. doi: 10.1186/cc11237. Crit Care. 2012. PMID: 22436665 Free PMC article.
References
-
- O'Grady NP, Barie PS, Bartlett JG, Bleck T, Carroll K, Kalil AC, Linden P, Maki DG, Nierman D, Pasculle W, Masur H. American College of Critical Care Medicine; Infectious Diseases Society of America. Guidelines for evaluation of new fever in critically ill adult patients: 2008 update from the American College of Critical Care Medicine and the Infectious Diseases Society of America. Crit Care Med. 2008;36:1330–1349. doi: 10.1097/CCM.0b013e318169eda9. - DOI - PubMed
-
- Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, Reinhart K, Angus DC, Brun-Buisson C, Beale R, Calandra T, Dhainaut JF, Gerlach H, Harvey M, Marini JJ, Marshall J, Ranieri M, Ramsay G, Sevransky J, Thompson BT, Townsend S, Vender JS, Zimmerman JL, Vincent JL. International Surviving Sepsis Campaign Guidelines Committee; American Association of Critical-Care Nurses; American College of Chest Physicians; American College of Emergency Physicians; Canadian Critical Care Society; European Society of Clinical Microbiology and Infectious Diseases; European Society of Intensive Care Medicine; European Respiratory Society; International Sepsis Forum; Japanese Association for Acute Medicine; Japanese Society of Intensive Care Medicine; Society of Critical Care Medicine; Society of Hospital Medicine; Surgical Infection Society; World Federation of Societies of Intensive and Critical Care Medicine. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med. 2008;36:296–327. doi: 10.1097/01.CCM.0000298158.12101.41. Erratum in: Crit Care Med 2008, 36:1394-1396. - DOI - PubMed
-
- Manthous CA, Hall JB, Olson D, Singh M, Chatila W, Pohlman A, Kushner R, Schmidt GA, Wood LD. Effect of cooling on oxygen consumption in febrile critically ill patients. Am J Respir Crit Care Med. 1995;151:10–14. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
