

Review of the principal extra spinal pathologies causing sciatica and new MRI approaches
- PMID: 22374280
- PMCID: PMC3474092
- DOI: 10.1259/bjr/84443179
Review of the principal extra spinal pathologies causing sciatica and new MRI approaches
Abstract
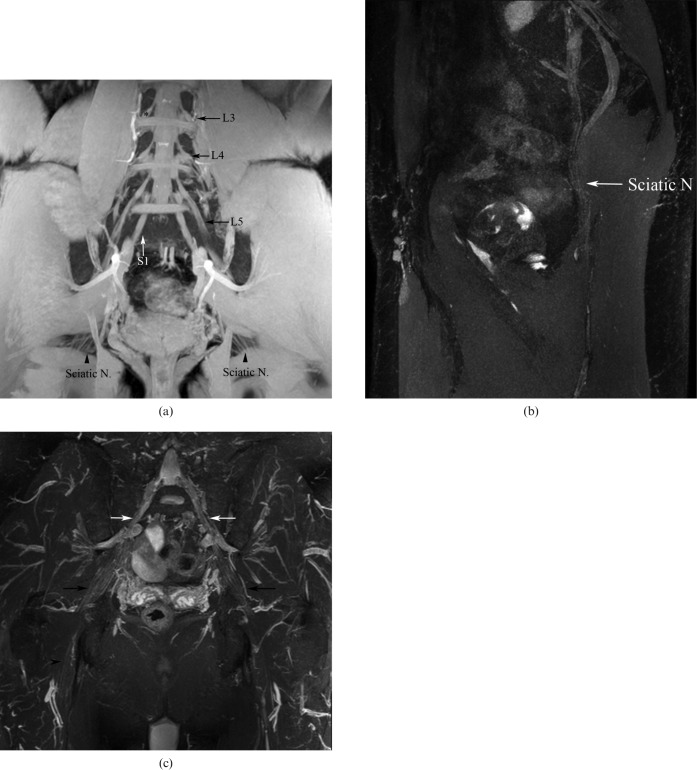
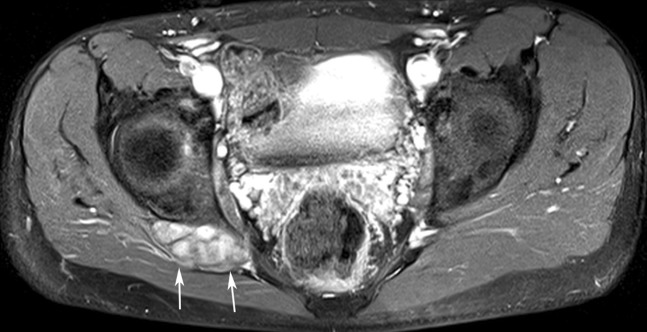
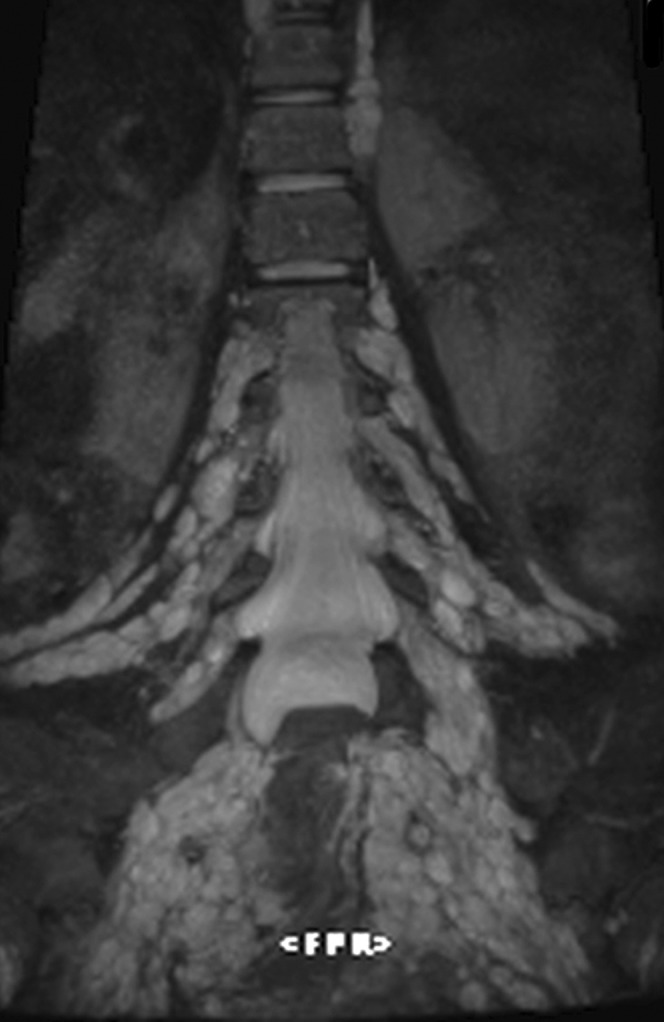
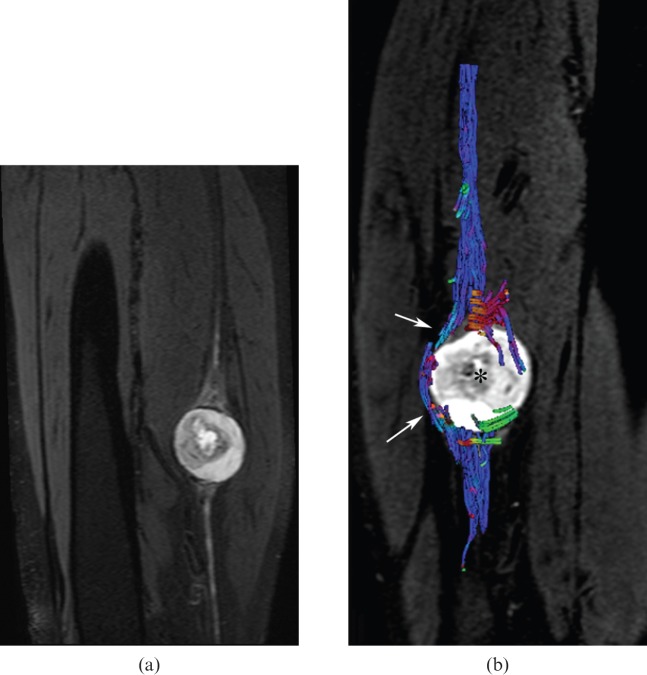
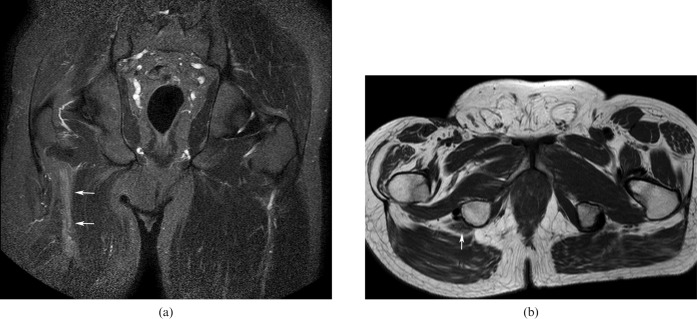
In this paper we illustrate the principal extraspinal pathologies causing sciatica and new approaches for the study of structures such as the lumbosacral plexus (LSP). Visualisation of the LSP in its entirety is difficult with conventional two-dimensional MRI sequences owing to its oblique orientation. In our institution, we have found that the utilisation of three-dimensional short tau inversion-recovery sampling perfection with application-optimised contrasts using different flip angle evolutions sequence is helpful, allowing multiplanar and maximum intensity projection reconstructions in the coronal oblique plane and curvilinear reformats through the plexus. Diffusion tensor imaging enables the observation of microstructural changes and can be useful in surgical planning. The normal anatomy of the LSP, its different extraspinal pathologies and differential diagnoses are thoroughly presented.
Figures
References
-
- Yoshimoto M, Kawaguchi S, Takebayashi T, Isogai S, Kurata Y, Nonaka S, et al. Diagnostic features of sciatica without lumbar nerve root compression. J Spinal Disord Tech 2008;22:328–33 - PubMed
-
- Rohkmann R. Atlas de Poche de neurologie. Paris, France: Flammarion; 2003
-
- Vargas MI, Beaulieu J, Magistris MR, Della Santa D, Delavelle J. Clinical findings, electroneuromyography and MRI in trauma of the brachial plexus. J Neuroradiol 2007;34:236–42 - PubMed
-
- Viallon M, Vargas MI, Jlassi H, Lövblad KO, Delavelle J. High-resolution and functional magnetic resonance imaging of the brachial plexus using an isotropic 3D T2 STIR (short term inversion recovery) SPACE sequence and diffusion tensor imaging. Eur Radiol 2008;18:1018–23 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
