

Fully covered self-expandable metal stents (SEMS), partially covered SEMS and self-expandable plastic stents for the treatment of benign esophageal ruptures and anastomotic leaks
- PMID: 22375711
- PMCID: PMC3313862
- DOI: 10.1186/1471-230X-12-19
Fully covered self-expandable metal stents (SEMS), partially covered SEMS and self-expandable plastic stents for the treatment of benign esophageal ruptures and anastomotic leaks
Abstract
Background: Benign esophageal ruptures and anastomotic leaks are life-threatening conditions that are often treated surgically. Recently, placement of partially and fully covered metal or plastic stents has emerged as a minimally invasive treatment option. We aimed to determine the clinical effectiveness of covered stent placement for the treatment of esophageal ruptures and anastomotic leaks with special emphasis on different stent designs.
Methods: Consecutive patients who underwent placement of a fully covered self-expandable metal stent (FSEMS), a partially covered SEMS (PSEMS) or a self-expanding plastic stent (SEPS) for a benign esophageal rupture or anastomotic leak after upper gastrointestinal surgery in the period 2007-2010 were included. Data on patient demographics, type of lesion, stent placement and removal, clinical success and complications were collected
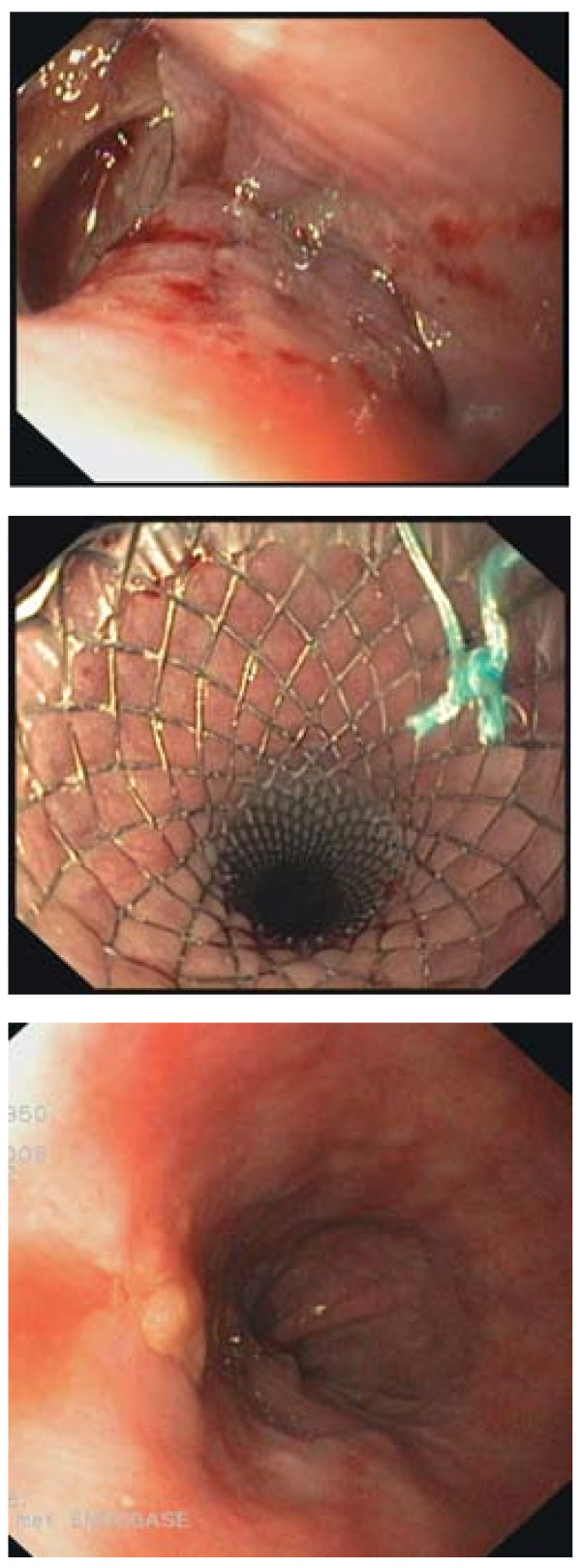
Results: A total of 52 patients received 83 esophageal stents (61 PSEMS, 15 FSEMS, 7 SEPS) for an anastomotic leak (n=32), iatrogenic rupture (n=13), Boerhaave's syndrome (n=4) or other cause (n=3). Endoscopic stent removal was successful in all but eight patients treated with a PSEMS due to tissue ingrowth. Clinical success was achieved in 34 (76%, intention-to-treat: 65%) patients (PSEMS: 73%, FSEMS: 83%, SEPS: 83%) after a median of 1 (range 1-5) stent and a median stenting time of 39 (range 7-120) days. In total, 33 complications in 24 (46%) patients occurred (tissue in- or overgrowth (n=8), stent migration (n=10), ruptured stent cover (all Ultraflex; n=6), food obstruction (n=3), severe pain (n=2), esophageal rupture (n=2), hemorrhage (n=2)). One (2%) patient died of a stent-related cause.
Conclusions: Covered stents placed for a period of 5-6 weeks may well be an alternative to surgery for treating benign esophageal ruptures or anastomotic leaks. As efficacy between PSEMS, FSEMS and SEPS is not different, stent choice should depend on expected risks of stent migration (SEPS and FSEMS) and tissue in- or overgrowth (PSEMS).
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
