

A double-blind, placebo-controlled trial of ruxolitinib for myelofibrosis
- PMID: 22375971
- PMCID: PMC4822164
- DOI: 10.1056/NEJMoa1110557
A double-blind, placebo-controlled trial of ruxolitinib for myelofibrosis
Abstract
Background: Ruxolitinib, a selective inhibitor of Janus kinase (JAK) 1 and 2, has clinically significant activity in myelofibrosis.
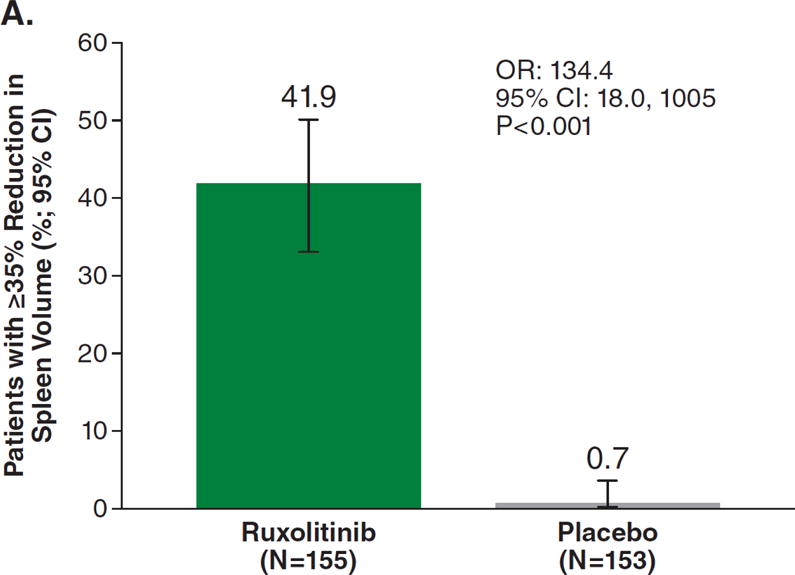
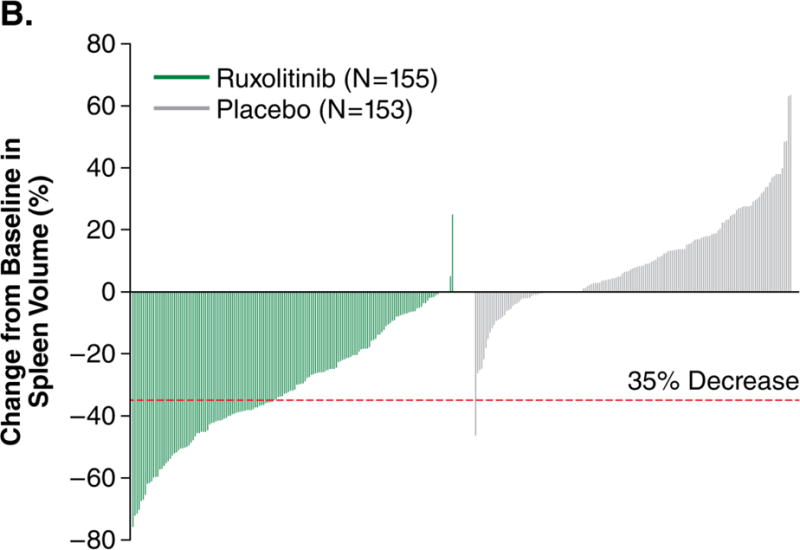
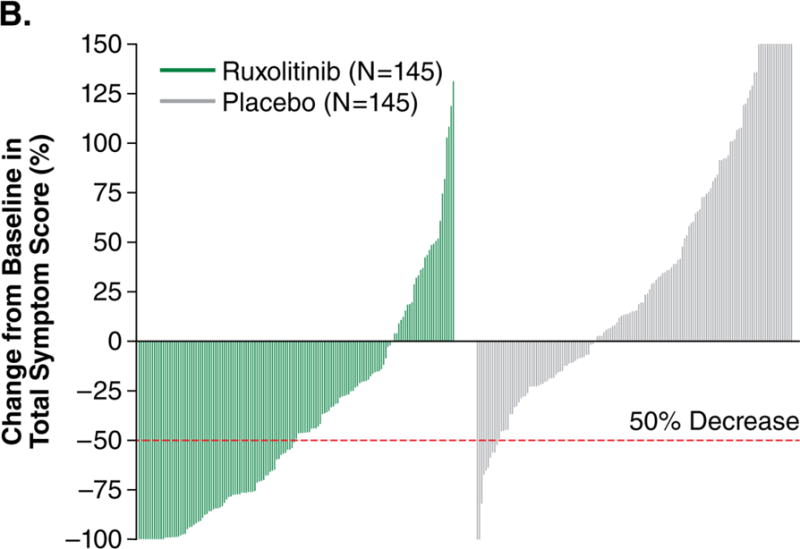
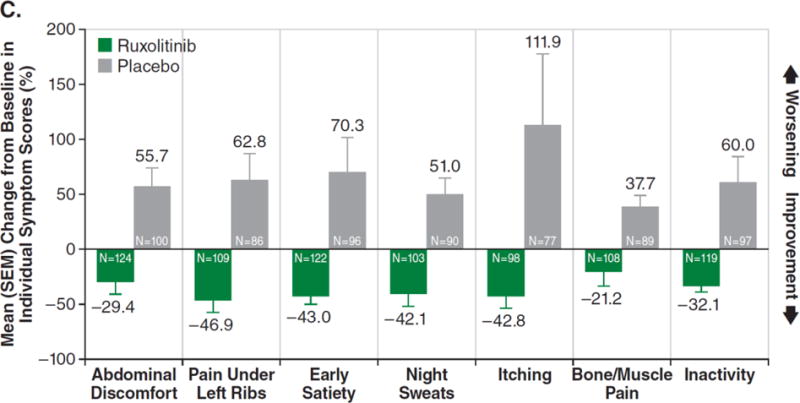
Methods: In this double-blind trial, we randomly assigned patients with intermediate-2 or high-risk myelofibrosis to twice-daily oral ruxolitinib (155 patients) or placebo (154 patients). The primary end point was the proportion of patients with a reduction in spleen volume of 35% or more at 24 weeks, assessed by means of magnetic resonance imaging. Secondary end points included the durability of response, changes in symptom burden (assessed by the total symptom score), and overall survival.
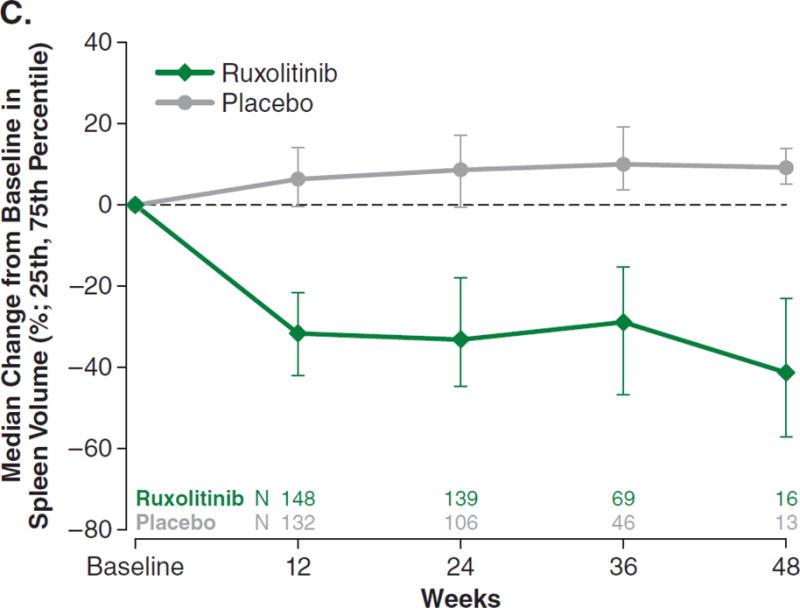
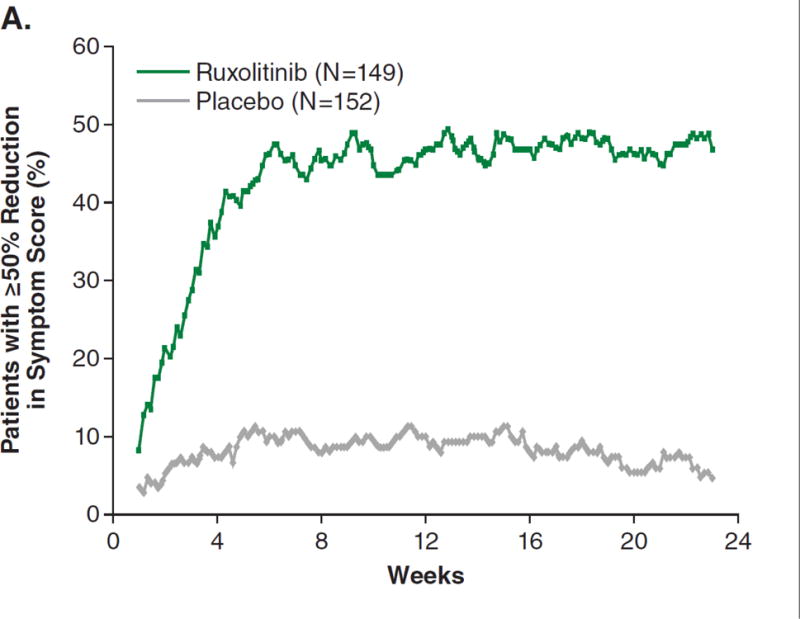
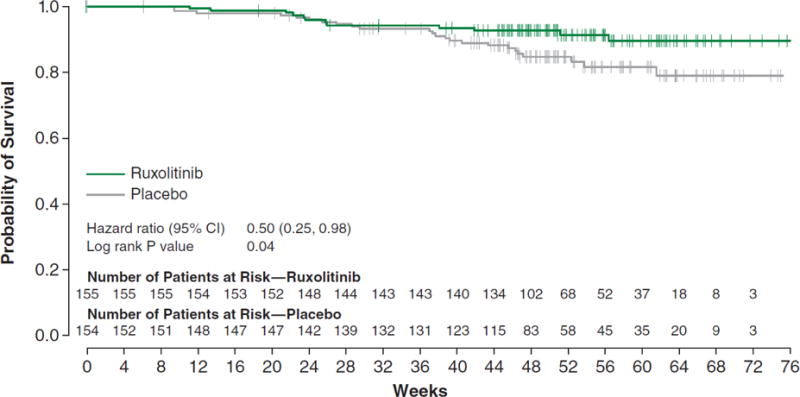
Results: The primary end point was reached in 41.9% of patients in the ruxolitinib group as compared with 0.7% in the placebo group (P<0.001). A reduction in spleen volume was maintained in patients who received ruxolitinib; 67.0% of the patients with a response had the response for 48 weeks or more. There was an improvement of 50% or more in the total symptom score at 24 weeks in 45.9% of patients who received ruxolitinib as compared with 5.3% of patients who received placebo (P<0.001). Thirteen deaths occurred in the ruxolitinib group as compared with 24 deaths in the placebo group (hazard ratio, 0.50; 95% confidence interval, 0.25 to 0.98; P=0.04). The rate of discontinuation of the study drug because of adverse events was 11.0% in the ruxolitinib group and 10.6% in the placebo group. Among patients who received ruxolitinib, anemia and thrombocytopenia were the most common adverse events, but they rarely led to discontinuation of the drug (in one patient for each event). Two patients had transformation to acute myeloid leukemia; both were in the ruxolitinib group.
Conclusions: Ruxolitinib, as compared with placebo, provided significant clinical benefits in patients with myelofibrosis by reducing spleen size, ameliorating debilitating myelofibrosis-related symptoms, and improving overall survival. These benefits came at the cost of more frequent anemia and thrombocytopenia in the early part of the treatment period. (Funded by Incyte; COMFORT-I ClinicalTrials.gov number, NCT00952289.).
Figures
Comment in
-
Challenges facing JAK inhibitor therapy for myeloproliferative neoplasms.N Engl J Med. 2012 Mar 1;366(9):844-6. doi: 10.1056/NEJMe1115119. N Engl J Med. 2012. PMID: 22375977 No abstract available.
-
Ruxolitinib for myelofibrosis.N Engl J Med. 2012 May 24;366(21):2032; author reply 2032-5. doi: 10.1056/NEJMc1203704. N Engl J Med. 2012. PMID: 22621635 No abstract available.
References
-
- Tefferi A, Vaidya R, Caramazza D, Finke C, Lasho T, Pardanani A. Circulating interleukin (IL)-8, IL-2R, IL-12, and IL-15 levels are independently prognostic in primary myelofibrosis: a comprehensive cytokine profiling study. J Clin Oncol. 2011;29:1356–63. - PubMed
-
- Cervantes F, Dupriez B, Pereira A, et al. New prognostic scoring system for primary myelofibrosis based on a study of the International Working Group for Myelofibrosis Research and Treatment. Blood. 2009;113:2895–901. - PubMed
-
- Abdel-Wahab OI, Levine RL. Primary myelofibrosis: update on definition, pathogenesis, and treatment. Annu Rev Med. 2009;60:233–45. - PubMed
-
- Delhommeau F, Jeziorowska D, Marzac C, Casadevall N. Molecular aspects of myeloproliferative neoplasms. Int J Hematol. 2010;91:165–73. - PubMed
-
- Vainchenker W, Dusa A, Constantinescu SN. JAKs in pathology: role of Janus kinases in hematopoietic malignancies and immunodeficiencies. Semin Cell Dev Biol. 2008;19:385–93. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials