

Cognitive changes following antidepressant or antipsychotic treatment in adolescents at clinical risk for psychosis
- PMID: 22377102
- PMCID: PMC3752907
- DOI: 10.1016/j.schres.2012.02.008
Cognitive changes following antidepressant or antipsychotic treatment in adolescents at clinical risk for psychosis
Abstract
Background: Improving neurocognitive abilities is a treatment priority in schizophrenia, however, pharmacological efforts to enhance deficits after illness onset have resulted in quite modest results that are of questionable clinical meaningfulness. Individuals at clinical risk for psychosis demonstrate neurocognitive impairments intermediate to the level of deficits observed in schizophrenia and normative performance, suggesting that a similar magnitude of improvement might result in more clinically meaningful change. In this study, we examined neurocognitive changes after six months of treatment in adolescents with clinical signs of risk for psychosis.
Methods: Adolescents who were referred to the Recognition and Prevention program, which is focused on treatment and research for individuals at a clinical high risk for psychosis, were followed in a naturalistic treatment design. At study entry and approximately six months after starting treatment, we examined neuropsychological functioning and clinical symptoms for patients who remained off medications (OFF; N=27), started selective serotonin reuptake inhibitor antidepressant medication (AD; N=15), or started a second-generation antipsychotic medication (AP; N=11) within three months of study entry. We also included a locally recruited healthy comparison group (HC; N=17).
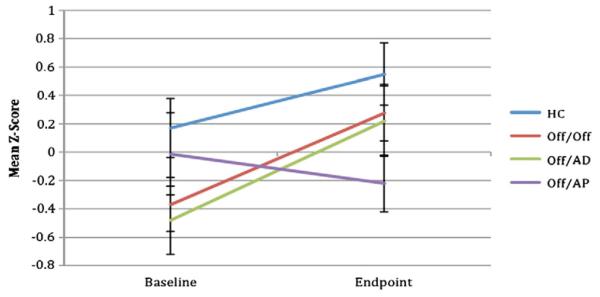
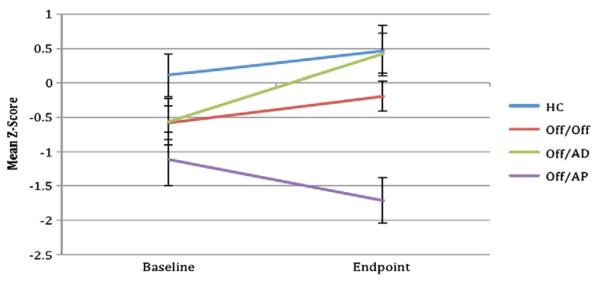
Results: The clinical groups were not significantly different on baseline demographic, neurocognitive, or clinical symptom measures. Linear mixed models were used to examine cognitive changes, with time between assessments, depressive symptom severity, and attenuated positive symptom severity as random effects. Group by time effects were observed in sustained attention and verbal learning, with the AD group showing a more favorable response than the AP group. The AD group's improvements were not significantly different from the HC or OFF group.
Conclusion: Early intervention for those at clinical high risk for psychosis may result in neurocognitive improvements. These improvements were observed for those prescribed antidepressant, but not antipsychotic medications even though the groups did not differ in clinical symptom severity or treatment response.
Copyright © 2012 Elsevier B.V. All rights reserved.
Figures
Similar articles
-
From the psychosis prodrome to the first-episode of psychosis: No evidence of a cognitive decline.J Psychiatr Res. 2018 Jan;96:231-238. doi: 10.1016/j.jpsychires.2017.10.014. Epub 2017 Oct 19. J Psychiatr Res. 2018. PMID: 29121595 Free PMC article. Clinical Trial.
-
Neurocognitive impairments in individuals at ultra-high risk for psychosis: Who will really convert?Aust N Z J Psychiatry. 2015 May;49(5):462-70. doi: 10.1177/0004867414561527. Epub 2014 Nov 25. Aust N Z J Psychiatry. 2015. PMID: 25425742
-
Cognitive neuropsychological functioning in New Zealand Māori diagnosed with schizophrenia.Aust N Z J Psychiatry. 2016 Jun;50(6):566-76. doi: 10.1177/0004867415607986. Epub 2015 Oct 22. Aust N Z J Psychiatry. 2016. PMID: 26494850
-
[Cognitive deficits in first episode psychosis patients and people at risk for psychosis: from diagnosis to treatment].Encephale. 2013 May;39 Suppl 1:S64-71. doi: 10.1016/j.encep.2012.10.011. Epub 2013 Mar 23. Encephale. 2013. PMID: 23528322 Review. French.
-
Memory deficits in children and adolescents with a psychotic disorder: a systematic review and meta-analysis.Eur Arch Psychiatry Clin Neurosci. 2025 Apr;275(3):715-732. doi: 10.1007/s00406-025-01961-w. Epub 2025 Feb 4. Eur Arch Psychiatry Clin Neurosci. 2025. PMID: 39903265
Cited by
-
The impact of psychosis on the course of cognition: a prospective, nested case-control study in individuals at clinical high-risk for psychosis.Psychol Med. 2015 Nov;45(15):3341-54. doi: 10.1017/S0033291715001233. Epub 2015 Jul 14. Psychol Med. 2015. PMID: 26169626 Free PMC article.
-
Evaluating the tendencies of community practitioners who actively practice in child and adolescent psychiatry to diagnose and treat DSM-5 attenuated psychotic syndrome.Eur Child Adolesc Psychiatry. 2022 Oct;31(10):1635-1644. doi: 10.1007/s00787-021-01897-1. Epub 2021 Oct 20. Eur Child Adolesc Psychiatry. 2022. PMID: 34669043
-
Is prevention a realistic goal for schizophrenia?Curr Psychiatry Rep. 2014 Apr;16(4):439. doi: 10.1007/s11920-014-0439-y. Curr Psychiatry Rep. 2014. PMID: 24566772 Review.
-
Longitudinal Cognitive Performance in Individuals at Ultrahigh Risk for Psychosis: A 10-year Follow-up.Schizophr Bull. 2019 Sep 11;45(5):1101-1111. doi: 10.1093/schbul/sby143. Schizophr Bull. 2019. PMID: 30321434 Free PMC article.
-
Clinical high risk for psychosis in children and adolescents: a systematic review.Eur Child Adolesc Psychiatry. 2018 Jun;27(6):683-700. doi: 10.1007/s00787-017-1046-3. Epub 2017 Sep 15. Eur Child Adolesc Psychiatry. 2018. PMID: 28914382
References
-
- Asarnow RF, Steffy RA, MacCrimmon DJ, Cleghorn JM. An attentional assessment of foster children at risk for schizophrenia. J. Abnorm. Psychol. 1977;86(3):267–275. - PubMed
-
- Beck AT, Steer RA, Garbin MG. Psychometric properties of the Beck Depression Inventory: twenty-five years of evaluation. Clin. Psychol. Rev. 1988;8(1):77–100.
-
- Benton A, Hamsher K, Sivan A. Multilingual Aphasia Examination. 3rd ed AJA Associates; Iowa City, Iowa: 1983.
-
- Bilder RM, Goldman RS, Robinson D, Reiter G, Bell L, Bates JA, et al. Neuropsychology of first-episode schizophrenia: initial characterization and clinical correlates. Am. J. Psychiatry. 2000;157(4):549–559. - PubMed
-
- Bowie CR, Reichenberg A, Patterson TL, Heaton RK, Harvey PD. Determinants of real-world functional performance in schizophrenia subjects: correlations with cognition, functional capacity, and symptoms. Am. J. Psychiatry. 2006;163(3):418–425. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
