

Seroprevalence of antibodies against Taenia solium cysticerci among refugees resettled in United States
- PMID: 22377408
- PMCID: PMC3309588
- DOI: 10.3201/eid1803.111367
Seroprevalence of antibodies against Taenia solium cysticerci among refugees resettled in United States
Abstract
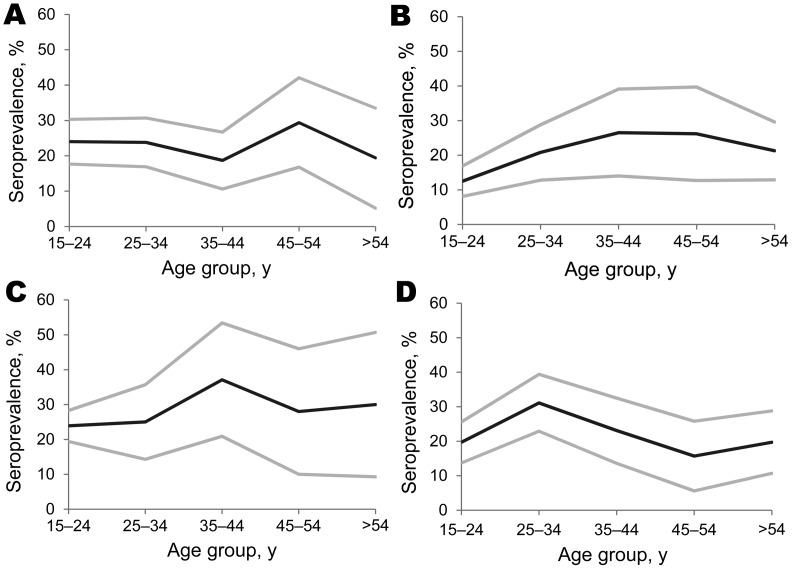
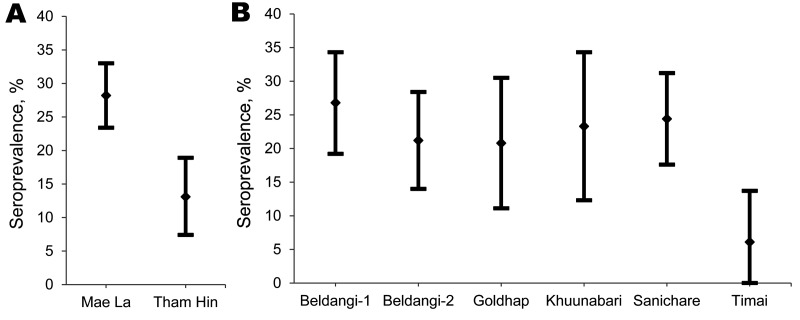
Neurocysticercosis (NCC) is a disease caused by central nervous system infection by the larval stage of the pork tapeworm, Taenia solium. In developing countries, NCC is a leading cause of adult-onset epilepsy. Case reports of NCC are increasing among refugees resettled to the United States and other nations, but the underlying prevalence among refugee groups is unknown. We tested stored serum samples from the Centers for Disease Control and Prevention Migrant Serum Bank for antibodies against T. solium cysts by using the enzyme-linked immunoelectrotransfer blot. Seroprevalence was high among all 4 populations tested: refugees from Burma (23.2%), Lao People's Democratic Republic (18.3%), Bhutan (22.8%), and Burundi (25.8%). Clinicians caring for refugee populations should suspect NCC in patients with seizure, chronic headache, or unexplained neurologic manifestations. Improved understanding of the prevalence of epilepsy and other associated diseases among refugees could guide recommendations for their evaluation and treatment before, during, and after resettlement.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources