

Masked hypertension and prehypertension: diagnostic overlap and interrelationships with left ventricular mass: the Masked Hypertension Study
- PMID: 22378035
- PMCID: PMC3668422
- DOI: 10.1038/ajh.2012.15
Masked hypertension and prehypertension: diagnostic overlap and interrelationships with left ventricular mass: the Masked Hypertension Study
Abstract
Background: Masked hypertension (MHT) and prehypertension (PHT) are both associated with an increase in cardiovascular disease (CVD) risk, relative to sustained normotension. This study examined the diagnostic overlap between MHT and PHT, and their interrelationships with left ventricular (LV) mass index (LVMI), a marker of cardiovascular end-organ damage.
Methods: A research nurse performed three manual clinic blood pressure (CBP) measurements on three occasions over a 3-week period (total of nine readings, which were averaged) in 813 participants without treated hypertension from the Masked Hypertension Study, an ongoing worksite-based, population study. Twenty-four-hour ambulatory blood pressure (ABP) was assessed by using a SpaceLabs 90207 monitor. LVMI was determined by echocardiography in 784 (96.4%) participants.
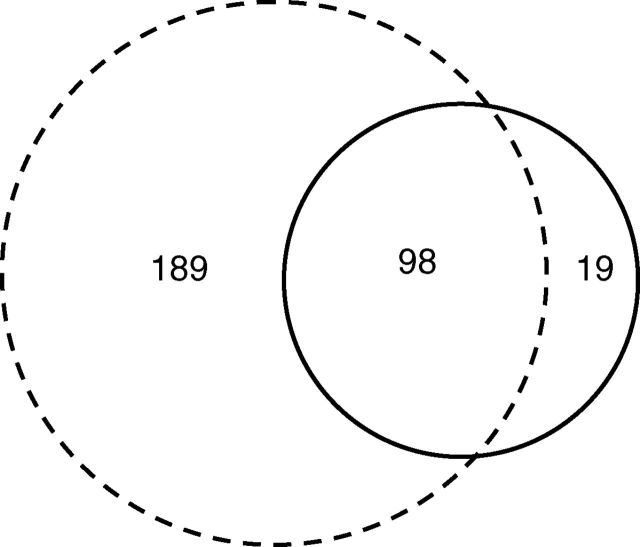
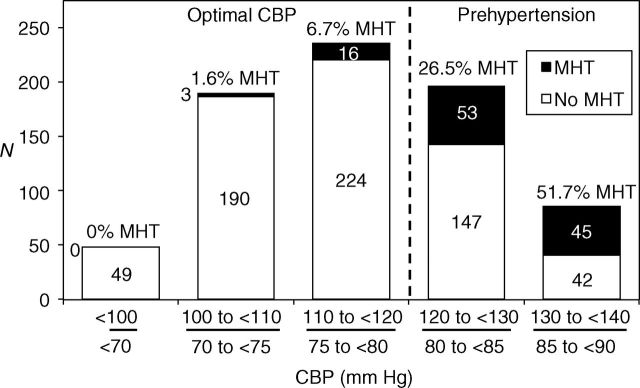
Results: Of the 813 participants, 769 (94.6%) had normal CBP levels (<140/90 mm Hg). One hundred and seventeen (15.2%) participants with normal CBP had MHT (normal CBP and mean awake ABP ≥135/85 mm Hg) and 287 (37.3%) had PHT (mean CBP 120-139/80-89 mm Hg). 83.8% of MHT participants had PHT and 34.1% of PHT participants had MHT. MHT was infrequent (3.9%) when CBP was optimal (<120/80 mm Hg). After adjusting for age, gender, body mass index (BMI), race/ethnicity, history of high cholesterol, history of diabetes, current smoking, family history of hypertension, and physical activity, compared with optimal CBP with MHT participants, LVMI was significantly greater in PHT without MHT participants and in PHT with MHT participants.
Conclusions: In this community sample, there was substantial diagnostic overlap between MHT and PHT. The diagnosis of MHT using an ABP monitor may not be warranted for individuals with optimal CBP.
Figures
Comment in
-
Are some "lone" atrial fibrillations caused by masked hypertension?Am J Hypertens. 2012 Aug;25(8):838. doi: 10.1038/ajh.2012.65. Am J Hypertens. 2012. PMID: 22820879 No abstract available.
References
-
- Pickering TG, Davidson K, Gerin W, Schwartz JE. Masked hypertension. Hypertension 2002;40:795–796 - PubMed
-
- Liu JE, Roman MJ, Pini R, Schwartz JE, Pickering TG, Devereux RB. Cardiac and arterial target organ damage in adults with elevated ambulatory and normal office blood pressure. Ann Intern Med 1999;131:564–572 - PubMed
-
- Björklund K, Lind L, Zethelius B, Andrén B, Lithell H. Isolated ambulatory hypertension predicts cardiovascular morbidity in elderly men. Circulation 2003;107:1297–1302 - PubMed
-
- Mancia G, Facchetti R, Bombelli M, Grassi G, Sega R. Long-term risk of mortality associated with selective and combined elevation in office, home, and ambulatory blood pressure. Hypertension 2006;47:846–853 - PubMed
-
- Ohkubo T, Kikuya M, Metoki H, Asayama K, Obara T, Hashimoto J, Totsune K, Hoshi H, Satoh H, Imai Y. Prognosis of “masked” hypertension and “white-coat” hypertension detected by 24-h ambulatory blood pressure monitoring 10-year follow-up from the Ohasama study. J Am Coll Cardiol 2005;46:508–515 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
