

A comparison of the effect of age on levator ani and obturator internus muscle cross-sectional areas and volumes in nulliparous women
- PMID: 22378544
- PMCID: PMC3624751
- DOI: 10.1002/nau.21208
A comparison of the effect of age on levator ani and obturator internus muscle cross-sectional areas and volumes in nulliparous women
Abstract
Aims: Functional tests have demonstrated minimal loss of vaginal closure force with age. So we tested the null hypotheses that age neither affects the maximum cross-sectional area (CSA) nor the volume of the levator muscle. Corresponding hypotheses were also tested in the adjacent obturator internus muscle, which served as a control for the effect of age on appendicular muscle in these women.
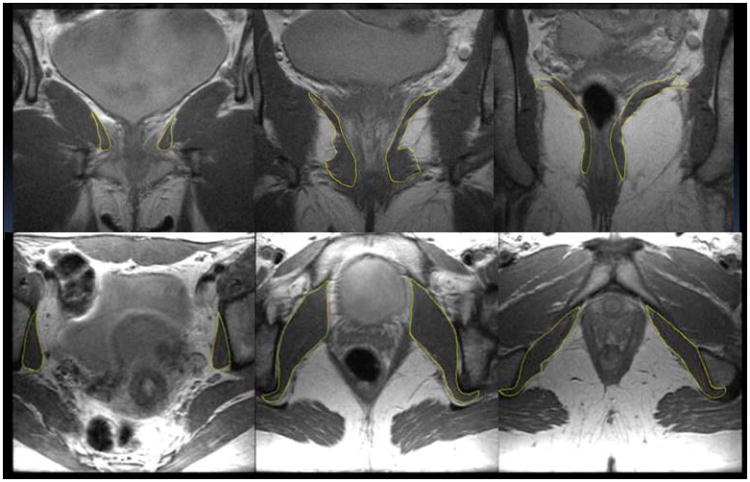
Methods: Magnetic resonance images of 15 healthy younger (aged 21-25 years) and 12 healthy older nulliparous women (aged >63 years) were selected to avoid the confounding effect of childbirth. Models were created from tracing outlines of the levator ani muscle in the coronal plane, and obturator internus in the axial plane using 3D Slicer v. 3.4. Muscle volumes were calculated using Slicer, while CSA was measured using Imageware™ at nine locations. The hypotheses were tested using repeated measures analysis of variance with P < 0.05 being considered significant.
Results: The effect of age did not reach statistical significance for the decrease in levator ani muscle maximum CSA or the decrease in volume (4.3%, P = 0.62 and 10.9%, 0.12, respectively). However, age did significantly adversely decrease obturator internus muscle maximum CSA and volume (24.5% and 28.2%, P < 0.001, respectively). Significant local age-related changes were observed dorsally in both muscles.
Conclusions: Unlike the adjacent appendicular muscle, obturator internus, the levator ani muscle in healthy nullipara does not show evidence of significant age-related atrophy.
Copyright © 2012 Wiley Periodicals, Inc.
Figures




References
-
- Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol. 1997;89:501–506. - PubMed
-
- Wu JM, Hundley AF, Fulton RG, Myers ER. Forecasting the prevalence of pelvic floor disorders in U.S. Women: 2010 to 2050. Obstet Gynecol. 2009;114:1278–1283. - PubMed
-
- Hoyte L, Jakab M, Warfield SK, Shott S, Flesh G, Fielding JR. Levator ani thickness variations in symptomatic and asymptomatic women using magnetic resonance-based 3-dimensional color mapping. Am J Obstet Gynecol. 2004;191:856–861. - PubMed
-
- Morgan DM, Kaur G, Hsu Y, Fenner DE, Guire K, Miller J, Ashton-Miller JA, DeLancey JOL. Does Vaginal Closure Force Differ in the Supine and Standing Positions. Am J Obstetr Gynecol. 2005;192:1722–1728. - PubMed
