

New acquisition of antibiotic-resistant organisms in skilled nursing facilities
- PMID: 22378900
- PMCID: PMC3347123
- DOI: 10.1128/JCM.06469-11
New acquisition of antibiotic-resistant organisms in skilled nursing facilities
Abstract
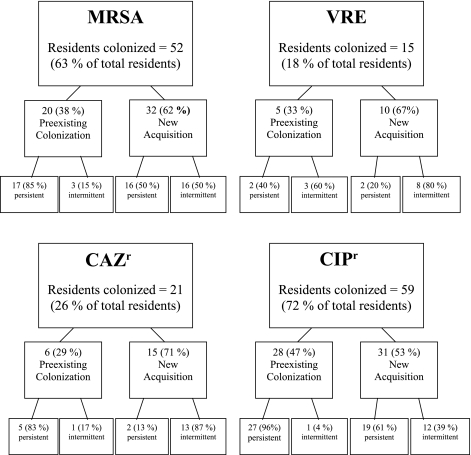
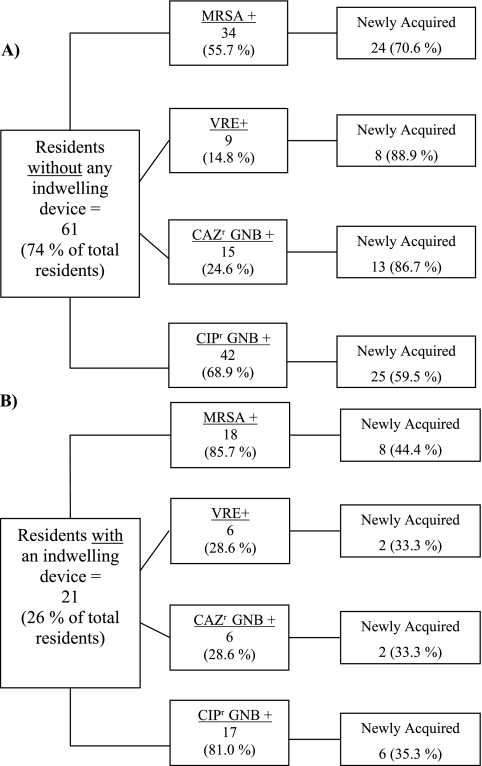
The epidemiology of new acquisition of antibiotic-resistant organisms (AROs) in community-based skilled nursing facilities (SNFs) is not well studied. To define the incidence, persistence of, and time to new colonization with methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci (VRE), and ceftazidime-resistant (CAZ(r)) and ciprofloxacin-resistant (CIP(r)) Gram-negative bacteria (GNB) in SNFs, SNF residents were enrolled and specimens from the nares, oropharynx, groin, perianal area, and wounds were prospectively cultured monthly. Standard microbiological tests were used to identify MRSA, VRE, and CAZ(r) and CIP(r) GNB. Residents with at least 3 months of follow-up were included in the analysis. Colonized residents were categorized as having either preexisting or new acquisition. The time to colonization for new acquisition of AROs was calculated. Eighty-two residents met the eligibility criteria. New acquisition of AROs was common. For example, of the 59 residents colonized with CIP(r) GNB, 28 (47%) were colonized with CIP(r) GNB at the start of the study (96% persistent and 4% intermittent), and 31 (53%) acquired CIP(r) GNB at the facility (61% persistent). The time to new acquisition was shortest for CIP(r) GNB, at a mean of 75.5 days; the time to new acquisition for MRSA was 126.6 days (P = 0.007 versus CIP(r) GNB), that for CAZ(r) was 176.0 days (P = 0.0001 versus CIP(r) GNB), and that for VRE was 186.0 days (P = 0.0004 versus CIP(r) GNB). Functional status was significantly associated with new acquisition of AROs (odds ratio [OR], 1.24; P = 0.01). New acquisition of AROs, in particular CIP(r) GNB and MRSA, is common in SNFs. CIP(r) GNB are acquired rapidly. Additional longitudinal studies to investigate risk factors for ARO acquisition are required.
Figures
References
-
- Anderson DJ, et al. 2008. Poor functional status as a risk factor for surgical site infection due to methicillin-resistant Staphylococcus aureus. Infect. Control Hosp. Epidemiol. 29:832–839 - PubMed
-
- Benenson S, et al. 2009. Vancomycin-resistant enterococci in long-term care facilities. Infect. Control Hosp. Epidemiol. 30:786–789 - PubMed
-
- Benoit SR, et al. 2008. Factors associated with antimicrobial use in nursing homes: a multilevel model. J. Am. Geriatr. Soc. 56:2039–2044 - PubMed
-
- Bonomo RA. 2000. Multiple antibiotic-resistant bacteria in long-term-care facilities: an emerging problem in the practice of infectious diseases. Clin. Infect. Dis. 31:1414–1422 - PubMed
-
- Bradley SF, et al. 1991. Methicillin-resistant Staphylococcus aureus: colonization and infection in a long-term care facility. Ann. Intern. Med. 115:417–422 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
