

State-of-the-art chronic thromboembolic pulmonary hypertension diagnosis and management
- PMID: 22379172
- PMCID: PMC9487476
- DOI: 10.1183/09059180.00009211
State-of-the-art chronic thromboembolic pulmonary hypertension diagnosis and management
Abstract
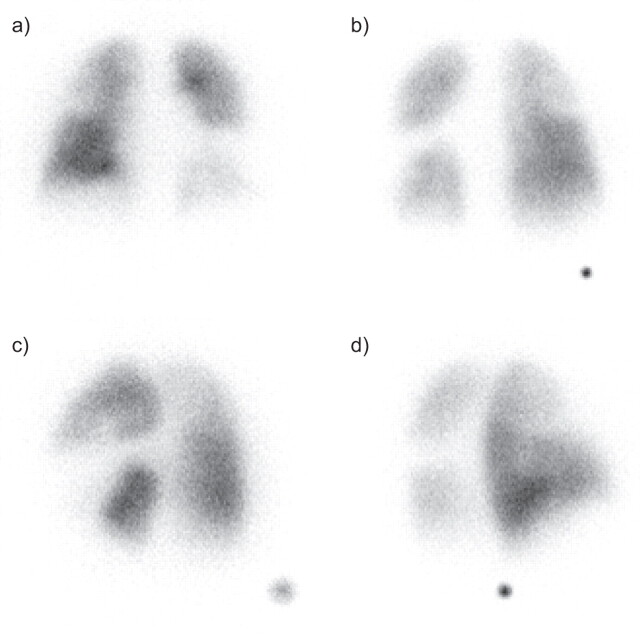
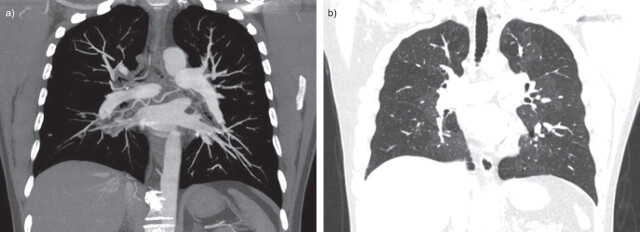
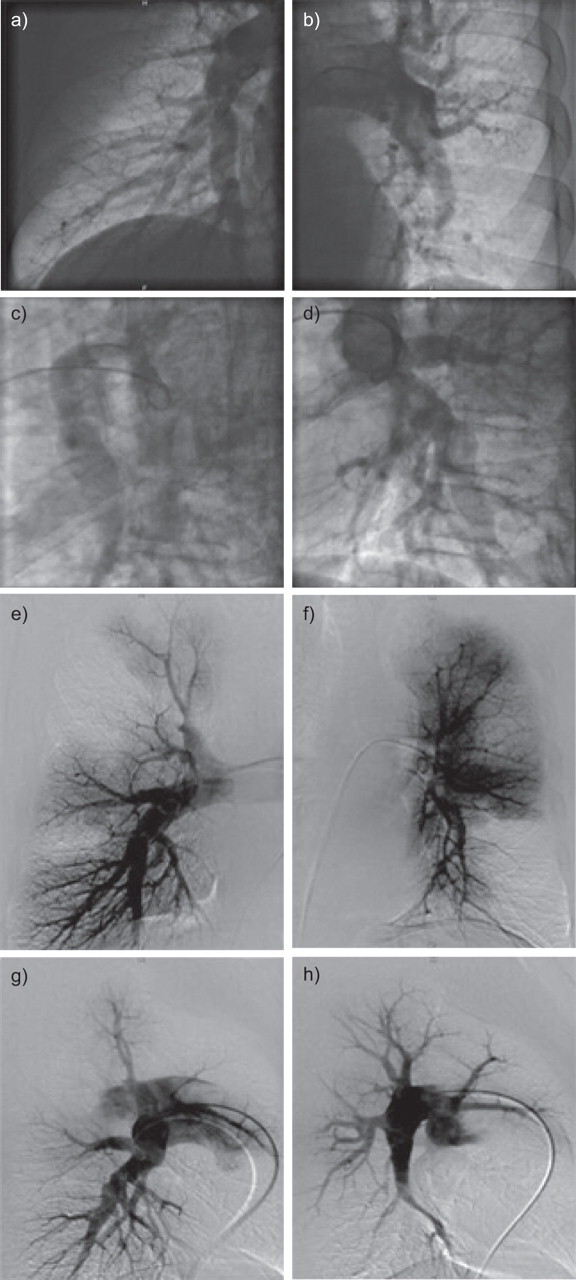
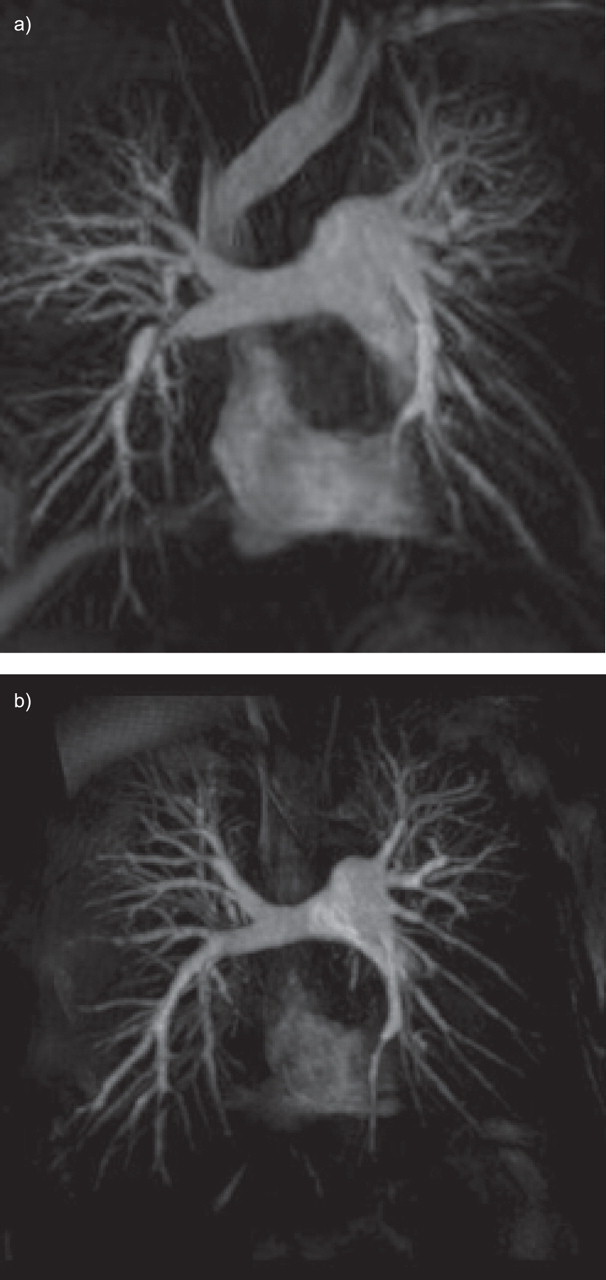
Chronic thromboembolic pulmonary hypertension (CTEPH) is a debilitating disease caused by chronic obstruction of pulmonary artery branches following episodes of pulmonary embolism and incomplete thrombus resolution. The prognosis of patients with CTEPH is poor unless an early diagnosis is made and treatment is initiated. Chest radiography and echocardiography are used in the initial assessment of suspected pulmonary hypertension. A diagnosis of CTEPH may be confirmed by the presence of a mismatched wedge-shaped perfusion deficit during ventilation/perfusion scintigraphy or characteristic findings during multi-slice computed tomography (CT) angiography, including a mosaic perfusion pattern, dilatation of proximal pulmonary arteries and right heart chambers, and the presence of vascular stenosis or obstruction. Prior to possible surgery, pulmonary angiography remains the definitive diagnostic technique, indicating the site and accessibility of the obstruction. However, many centres utilise CT and magnetic resonance imaging following recent advances in these noninvasive techniques. Haemodynamic evaluation via right heart catheterisation is also mandatory, as pulmonary vascular resistance is the most important determinant of both prognosis and the risk associated with pulmonary endarterectomy surgery. Accurate CTEPH diagnosis and characterisation of its extent and distribution are imperative to allow the prompt initiation of treatment, particularly surgical pulmonary endarterectomy in eligible patients.
Conflict of interest statement
E. Mayer has received fees for speaking and consultancy from Actelion and Bayer Pharma.
Figures
References
-
- Moser KM, Auger WR, Fedullo PF. Chronic major-vessel thromboembolic pulmonary hypertension. Circulation 1990; 81: 1735–1743. - PubMed
-
- Dalen JE, Alpert JS. Natural history of pulmonary embolism. Prog Cardiovasc Dis 1975; 17: 259–270. - PubMed
-
- Jamieson SW, Kapelanski DP, Sakakibara N, et al. . Pulmonary endarterectomy: experience and lessons learned in 1,500 cases. Ann Thorac Surg 2003; 76: 1457–1462. - PubMed
-
- D'Armini AM, Cattadori B, Monterosso C, et al. . Pulmonary thromboendarterectomy in patients with chronic thromboembolic pulmonary hypertension: hemodynamic characteristics and changes. Eur J Cardiothorac Surg 2000; 18: 696–701. - PubMed
-
- Pepke-Zaba J, Delcroix M, Lang I, et al. . Chronic thromboembolic pulmonary hypertension (CTEPH): results from an international prospective registry. Circulation 2011; 124: 1973–1981. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical