

AASM criteria for scoring respiratory events: interaction between apnea sensor and hypopnea definition
- PMID: 22379249
- PMCID: PMC3274344
- DOI: 10.5665/sleep.1710
AASM criteria for scoring respiratory events: interaction between apnea sensor and hypopnea definition
Abstract
Study objectives: To examine the impact of using a nasal pressure sensor only vs the American Academy of Sleep Medicine (AASM) recommended combination of thermal and nasal pressure sensors on (1) the apnea index (AI), (2) the apnea-hypopnea index (AHI), where the AHI is calculated using both AASM definitions of hypopnea, and (3) the accuracy of a diagnosis of obstructive sleep apnea (OSA).
Design: Retrospective review of previously scored in-laboratory polysomnography.
Setting: A tertiary-hospital clinical sleep laboratory.
Patients or participants: One hundred sixty-four consecutive adult patients with a potential diagnosis of OSA, who were examined during a 3-month period.
Interventions: N/A.
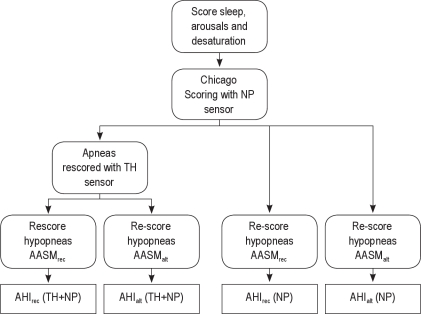
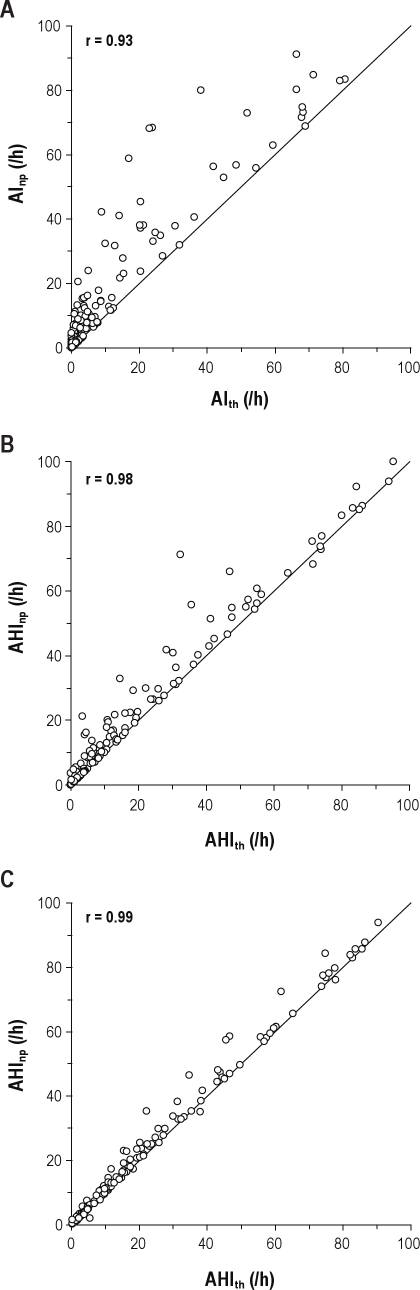
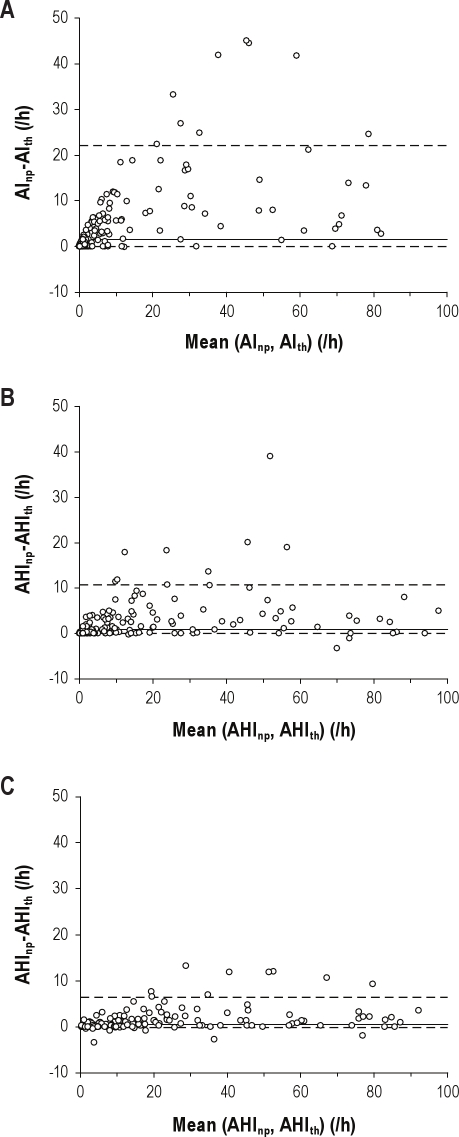
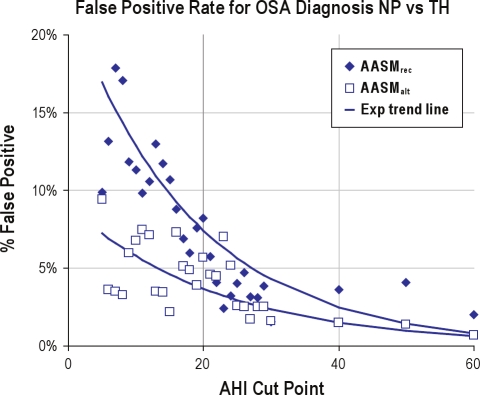
Measurements and results: Studies were scored with and without the use of the oronasal thermal sensor. AIs and AHIs, using the nasal pressure sensor alone (AI(np) and AHI(np)), were compared with those using both a thermal sensor for the detection of apnea and a nasal pressure transducer for the detection of hypopnea (AI(th) and AHI(th)). Comparisons were repeated using the AASM recommended (AASM(rec)) and alternative (AASM(alt)) hypopnea definitions. AI was significantly different when measured from the different sensors, with AI(np) being 51% higher on average. Using the AASM(rec) hypopnea definition, the mean AHI(np) was 15% larger than the AHI(th); with large interindividual differences and an estimated 9.8% of patients having a false-positive OSA diagnosis at a cutpoint of 15 events and 4.3% at 30 events per hour. Using AASM(alt) hypopnea definition, the mean AHI(np) was 3% larger than the AHI(th), with estimated false-positive rates of 4.6% and 2.4%, respectively. The false-negative rate was negligible at 0.1% for both hypopnea definitions.
Conclusions: This study demonstrates that using only a nasal pressure sensor for the detection of apnea resulted in higher values of AI and AHI than when the AASM recommended thermal sensor was added to detect apnea. When the AASM(alt) hypopnea definition was used, the differences in AHI and subsequent OSA diagnosis were small and less than when the AASM(rec) hypopnea definition was used. In situations in which a thermal sensor cannot be used, for example, in limited-channel diagnostic devices, the AHI obtained with a nasal pressure sensor alone differs less from the AHI obtained from a polysomnogram that includes a thermal sensor when the AASM(alt) definition rather than the AASM(rec) definition of hypopnea is used. Thus, diagnostic accuracy is impacted both by the absence of the thermal sensor and by the rules used to analyze the polysomnography. Furthermore, where the thermal sensor is unreliable for sections of a study, it is likely that use of the nasal pressure signal to detect apnea will have modest impact.
Keywords: AASM guidelines; apnea; diagnosis; hypopnea; methodology; nasal pressure sensor; obstructive sleep apnea; polysomnography; scoring; sleep disordered breathing; thermal sensor.
Figures
Similar articles
-
The new AASM criteria for scoring hypopneas: impact on the apnea hypopnea index.Sleep. 2009 Feb;32(2):150-7. doi: 10.1093/sleep/32.2.150. Sleep. 2009. PMID: 19238801 Free PMC article.
-
Rules for scoring respiratory events in sleep: update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine.J Clin Sleep Med. 2012 Oct 15;8(5):597-619. doi: 10.5664/jcsm.2172. J Clin Sleep Med. 2012. PMID: 23066376 Free PMC article.
-
Impact of AASM 2012 Recommended Hypopnea Criteria on Surgical Outcomes for Obstructive Sleep Apnea.Laryngoscope. 2020 Mar;130(3):825-831. doi: 10.1002/lary.28019. Epub 2019 Apr 29. Laryngoscope. 2020. PMID: 31034617 Clinical Trial.
-
The AASM scoring manual: a critical appraisal.Curr Opin Pulm Med. 2009 Nov;15(6):540-9. doi: 10.1097/MCP.0b013e328331a2bf. Curr Opin Pulm Med. 2009. PMID: 19738470 Review.
-
Obstructive sleep apnea devices for out-of-center (OOC) testing: technology evaluation.J Clin Sleep Med. 2011 Oct 15;7(5):531-48. doi: 10.5664/JCSM.1328. J Clin Sleep Med. 2011. PMID: 22003351 Free PMC article. Review.
Cited by
-
Mandibular advancement device versus CPAP in lowering 24-hour blood pressure in patients with obstructive sleep apnoea and hypertension: the CRESCENT trial protocol.BMJ Open. 2023 May 31;13(5):e072853. doi: 10.1136/bmjopen-2023-072853. BMJ Open. 2023. PMID: 37258080 Free PMC article.
-
Performance of instruments aimed at detecting obstructive sleep apnea syndrome among individuals in Chile.J Bras Pneumol. 2019 Dec 13;46(1):e20190015. doi: 10.1590/1806-3713/e20190015. J Bras Pneumol. 2019. PMID: 31851221 Free PMC article. No abstract available.
-
Home-based diagnosis of obstructive sleep apnea in an urban population.J Clin Sleep Med. 2014 Aug 15;10(8):879-85. doi: 10.5664/jcsm.3960. J Clin Sleep Med. 2014. PMID: 25126034 Free PMC article. Clinical Trial.
-
Combination mode of physiological signals for diagnosis of OSAS using portable monitor.Sleep Breath. 2018 Mar;22(1):123-129. doi: 10.1007/s11325-017-1544-z. Epub 2017 Jul 26. Sleep Breath. 2018. PMID: 28744805 Clinical Trial.
-
Deep learning for obstructive sleep apnea diagnosis based on single channel oximetry.Nat Commun. 2023 Aug 12;14(1):4881. doi: 10.1038/s41467-023-40604-3. Nat Commun. 2023. PMID: 37573327 Free PMC article.
References
-
- Iber C, Ancoli-Israel S, Chesson A, Quan S for the American Academy of Sleep Medicine. 1st ed. Westchester, IL: American Academy of Sleep Medicine; 2007. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications.
-
- Parrino L, Ferri R, Zucconi M, Fanfulla F. Commentary from the Italian Association of Sleep Medicine on the AASM manual for the scoring of sleep and related events: For debate and discussion. Sleep Med. 2009;10:799–808. - PubMed
-
- Lee-Chiong T. New Sleep Scoring Guidelines. American College of Chest Physicians: Pulmonary, Critical Care, Sleep Update. [Accessed: October 26, 2011];2008 Volume 22 Available at: http://www.chestnet.org/accp/pccsu/new-sleep-scoring-guidelines?page=0,3.
-
- Cardozo JS. New AASM recommendations for sensors: a simple guide for the sleep technologist. Sleep Diagnosis Therap. 2008;3:21.
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
