

Thoracic duct embolization for chylous leaks
- PMID: 22379277
- PMCID: PMC3140251
- DOI: 10.1055/s-0031-1273941
Thoracic duct embolization for chylous leaks
Abstract
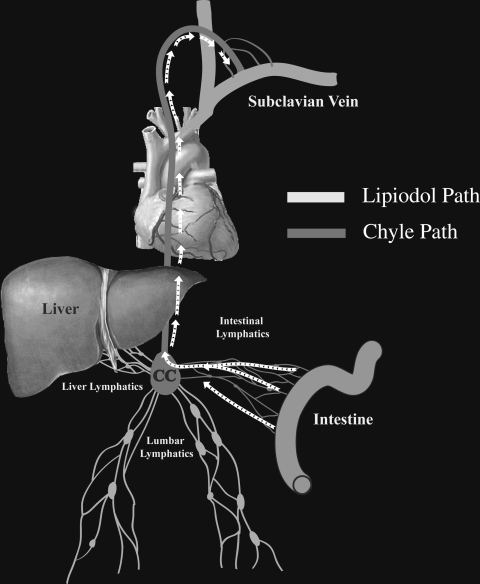
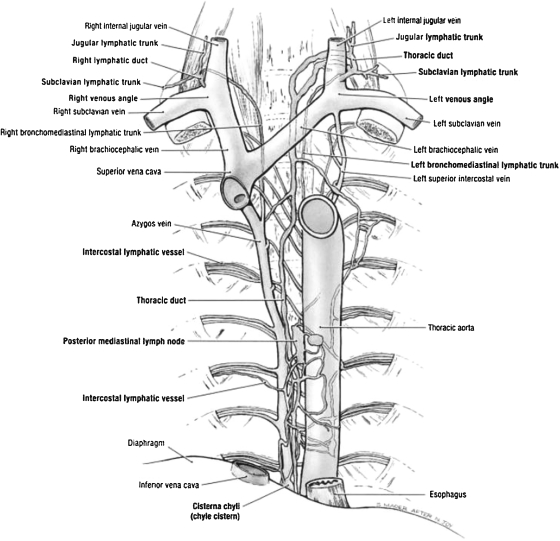
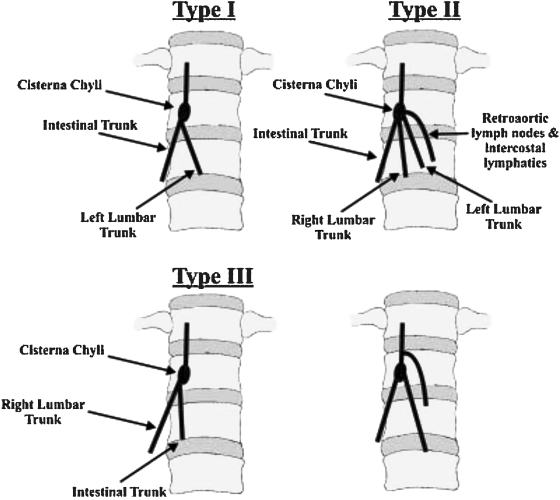
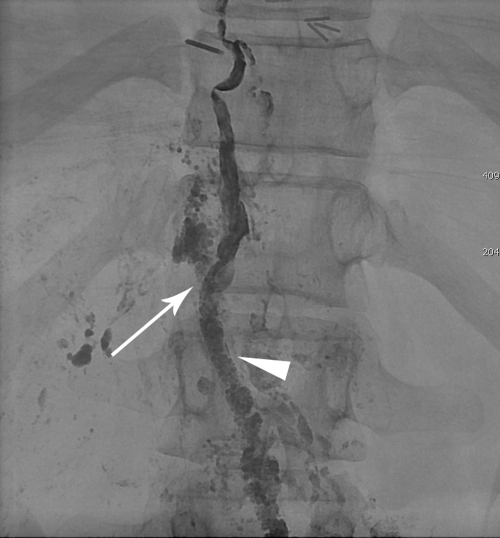
Chylous leaks, such as chylothorax and chylopericardium, are uncommon effusions resulting from the leakage of intestinal lymphatic fluid from the thoracic duct (TD) and its tributaries, or intestinal lymphatic ducts. The cause can be either traumatic (thoracic surgery) or nontraumatic (idiopathic, malignancy). Treatment has traditionally consisted of dietary modification (nonfat diet) and/or surgery (TD ligation, pleurodesis). Thoracic duct embolization (TDE) has become a viable treatment alternative due to it high success rate and minimal complications. In this article, the authors describe the etiologies of chylothorax, patient population, outcomes, and long-term follow-up of TDE patients. Relevant lymphatic anatomy and physiology are reviewed, with special attention paid to the formation of the duct by tributaries at the cisterna chyli (CC). The technique of TDE is outlined, including bilateral pedal lymphangiography, TD cannulation, and embolic agents used for the procedure.
Keywords: Thoracic duct embolization; chyle leak; chylothorax.
Figures
References
-
- Dunn R P. Primary chylopericardium: a review of the literature and an illustrated case. Am Heart J. 1975;89(3):369–377. - PubMed
-
- Itkin M, Swe N M, Shapiro S E, Shrager J B. Spontaneous chylopericardium: delineation of the underlying anatomic pathology by CT lymphangiography. Ann Thorac Surg. 2009;87(5):1595–1597. - PubMed
-
- Doerr C H, Allen M S, Nichols F C, III, Ryu J H. Etiology of chylothorax in 203 patients. Mayo Clin Proc. 2005;80(7):867–870. - PubMed
-
- Cerfolio R J, Allen M S, Deschamps C, Trastek V F, Pairolero P C. Postoperative chylothorax. J Thorac Cardiovasc Surg. 1996;112(5):1361–1365. discussion 1365–1366. - PubMed
-
- Dougenis D, Walker W S, Cameron E W, Walbaum P R. Management of chylothorax complicating extensive esophageal resection. Surg Gynecol Obstet. 1992;174(6):501–506. - PubMed
