

Anorectal infection: abscess-fistula
- PMID: 22379401
- PMCID: PMC3140329
- DOI: 10.1055/s-0031-1272819
Anorectal infection: abscess-fistula
Abstract
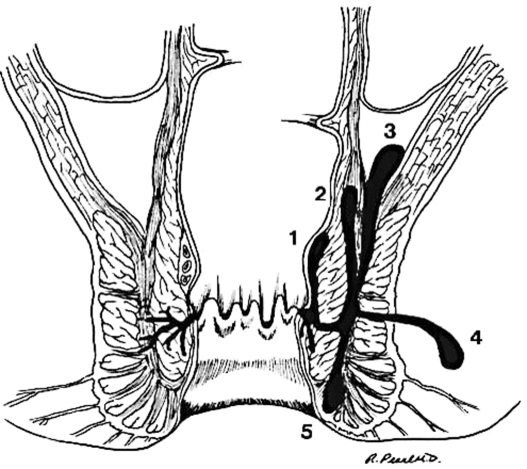
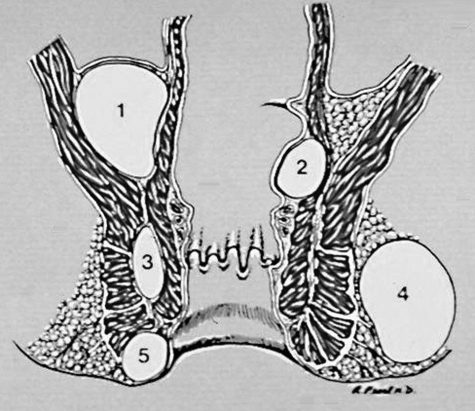
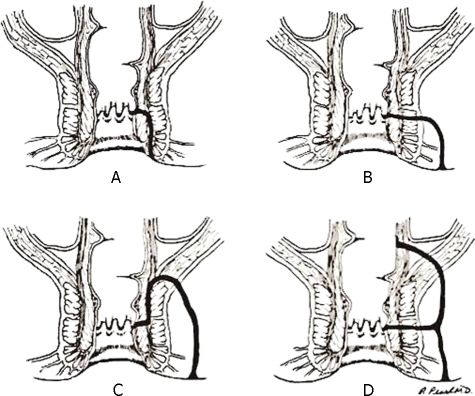
Anorectal abscess and fistula are among the most common diseases encountered in adults. Abscess and fistula should be considered the acute and chronic phase of the same anorectal infection. Abscesses are thought to begin as an infection in the anal glands spreading into adjacent spaces and resulting in fistulas in ~40% of cases. The treatment of an anorectal abscess is early, adequate, dependent drainage. The treatment of a fistula, although surgical in all cases, is more complex due to the possibility of fecal incontinence as a result of sphincterotomy. Primary fistulotomy and cutting setons have the same incidence of fecal incontinence depending on the complexity of the fistula. So even though the aim of a surgical procedure is to cure a fistula, conservative management short of major sphincterotomy is warranted to preserve fecal incontinence. However, trading radical surgery for conservative (nonsphincter cutting) procedures such as a draining seton, fibrin sealant, anal fistula plug, endorectal advancement flap, dermal island flap, anoplasty, and LIFT (ligation of intersphincteric fistula tract) procedure all result in more recurrence/persistence requiring repeated operations in many cases. A surgeon dealing with fistulas on a regular basis must tailor various operations to the needs of the patient depending on the complexity of the fistula encountered.
Keywords: Fistula; abscess; anorectal infection; fecal incontinence; sphincterotomy.
Figures
References
-
- Shrum R C. Anorectal pathology in 1000 consecutive patients with suspected surgical disorders. Dis Colon Rectum. 1959;2:469–472. - PubMed
-
- Buda A M. General candidates of fistula in ano: the role of foreign bodies as causative factors fistulas. Am J Surg. 1941;54:384–387.
-
- Buie S L., Sr Practice Proctology. 2nd ed. Springfield, IL: Charles C Thomas; 1960.
-
- Sainio P. Fistula in ano in a defined population: incidence and epidemiology of patients. Ann Chir Gynaecol. 1984;73:219–224. - PubMed
-
- Nelson R L. Anorectal abscess fistula: what do we know? Surg Clin North Am. 2002;82(6):1139–1151. v–vi. - PubMed
LinkOut - more resources
Full Text Sources
