

doi: 10.1055/s-0031-1272823.
Pilonidal disease
Affiliations
- PMID: 22379405
- PMCID: PMC3140333
- DOI: 10.1055/s-0031-1272823
Item in Clipboard
Pilonidal disease
Clin Colon Rectal Surg.
2011 Mar.
Abstract
Pilonidal disease presents many therapeutic challenges to surgeons throughout the world. Its varied clinical presentations necessitate a wide range of treatments, thus underscoring the need to tailor the treatment to the patient and the severity of disease. Recent studies confirm the efficacy of smaller, more conservative operations for appropriate indications. When flap closures are performed, every attempt should be directed to placing sutures off (lateral) to the midline gluteal cleft. Meticulous attention to the details of immediate and long-term postoperative care is paramount.
Keywords: Bascom cleft lift; Karydakis flap; Pilonidal disease; abscess.
Figures
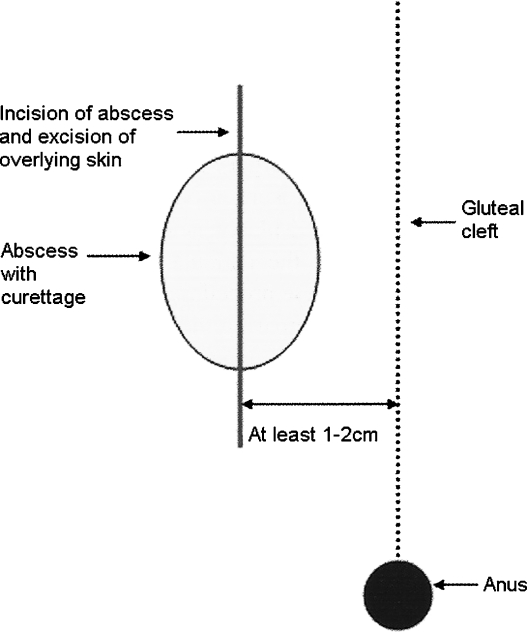
Off-midline incision and drainage of pilonidal abscess. Lateral incision for drainage is made even when the abscess is primarily in the midline. Modified from Nelson and Billingham.
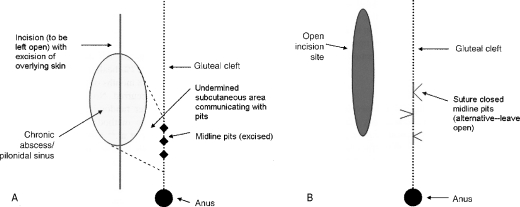
(A) Bascom lateral drainage. (B) Subcutaneous undermining and excision of sinus pits. Modified from Nelson and Billingham.
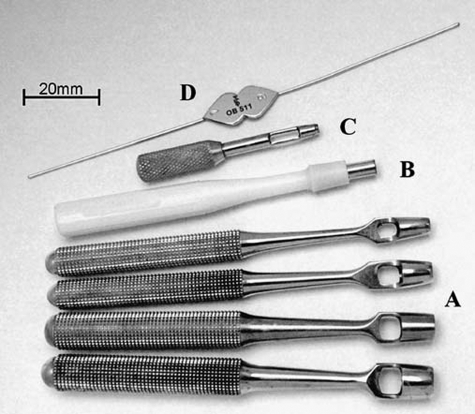
(A) Keyes trephines of various diameters. (B) Disposable punch. (C) Ophthalmic Searcy trephine. (D) Thin lacrimal 0/00 probe. From Gips et al. With permission from Wolters Kluwer Health.
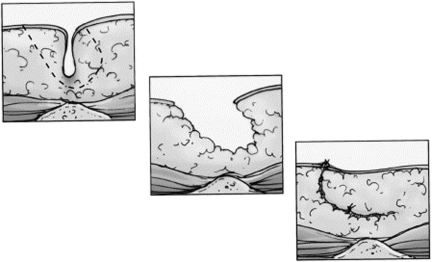
Excision of the disease and primary closure is one surgical option. In an effort to improve upon this technique, Karydakis modified the procedure. The midline sinus is excised elliptically and the wound closed lateral to the midline. To do this, a thick flap is created by undercutting the medial wound edge and advancing it across the midline. By doing this, the natal cleft is flattened and the entire suture line is positioned lateral to the midline. From Hull and Wu. With permission from Elsevier.
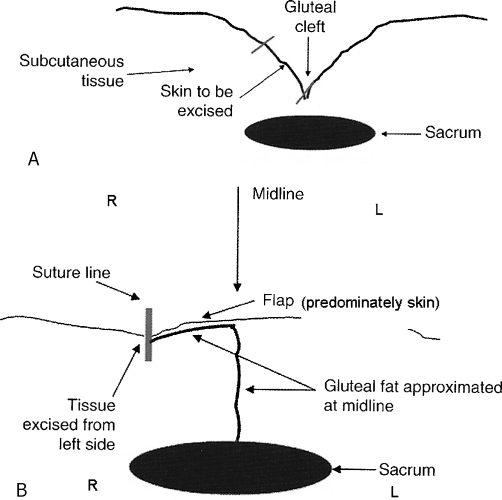
(A) Cleft lift technique as described by Bascom (Bascom II) for nonhealing midline wounds. (B) Final result after flap is raised and underlying gluteal fat is approximated. Modified from Nelson and Billingham.
References
-
- Søndenaa K, Andersen E, Nesvik I, Søreide J A. Patient characteristics and symptoms in chronic pilonidal sinus disease. Int J Colorectal Dis. 1995;10(1):39–42. - PubMed
-
- Akinci O F, Bozer M, Uzunköy A, Düzgün S A, Coşkun A. Incidence and aetiological factors in pilonidal sinus among Turkish soldiers. Eur J Surg. 1999;165(4):339–342. - PubMed
-
- Hodges R M. Pilo-nidal sinus. Boston Med Surg J. 1880;103:485–486.
-
- Buie L A. Jeep disease. South Med J. 1944;37:103–109.
LinkOut - more resources
Full Text Sources
Other Literature Sources
