

Multisegmental foot and ankle motion analysis after hallux valgus surgery
- PMID: 22381346
- PMCID: PMC4612516
- DOI: 10.3113/FAI.2012.0141
Multisegmental foot and ankle motion analysis after hallux valgus surgery
Abstract
Background: Gait changes in patients with hallux valgus, including altered kinematic and temporal-spatial parameters, have been documented in the literature. Although operative treatment can yield favorable clinical and radiographic results, restoration of normal gait in this population remains unclear. Segmental kinematic changes within the foot and ankle during ambulation after operative correction of hallux valgus have not been reported. The aim of this study was to analyze changes in multisegmental foot and ankle kinematics in patients who underwent operative correction of hallux valgus.
Methods: A 15-camera Vicon Motion Analysis System was used to evaluate 24 feet in 19 patients with hallux valgus preoperatively and postoperatively. The Milwaukee Foot Model was used to characterize segmental kinematics and temporal-spatial parameters (TSPs). Preoperative and postoperative kinematics and TSPs were compared using paired nonparametric methods; comparisons with normative data were performed using unpaired nonparametric methods. Outcomes were evaluated using the SF-36 assessment tool.
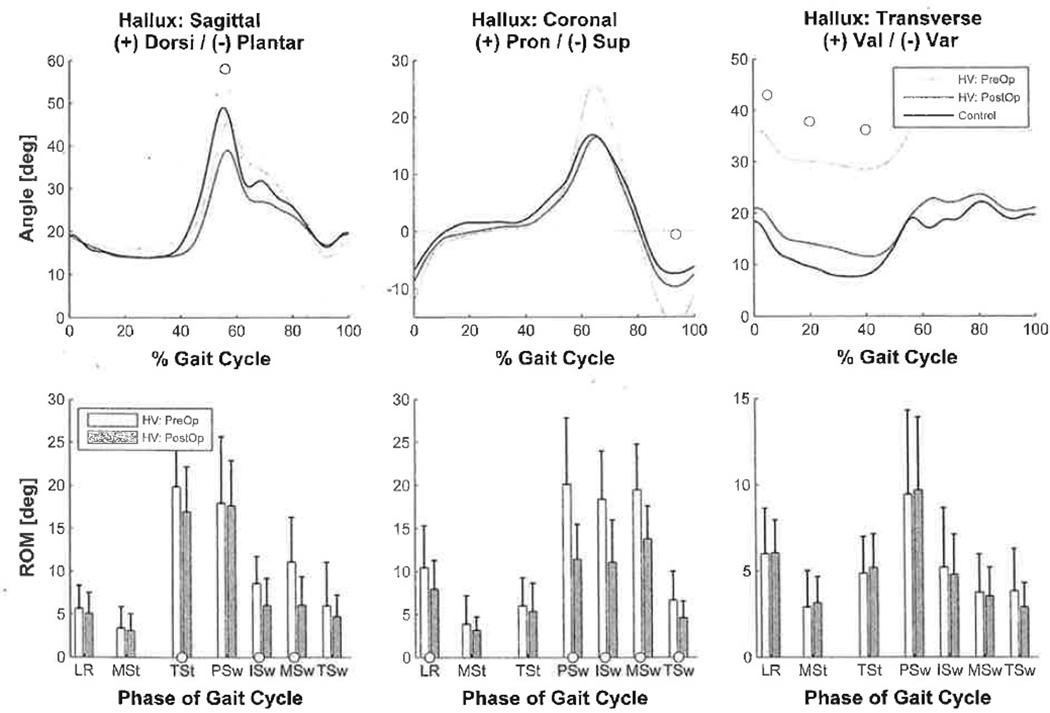
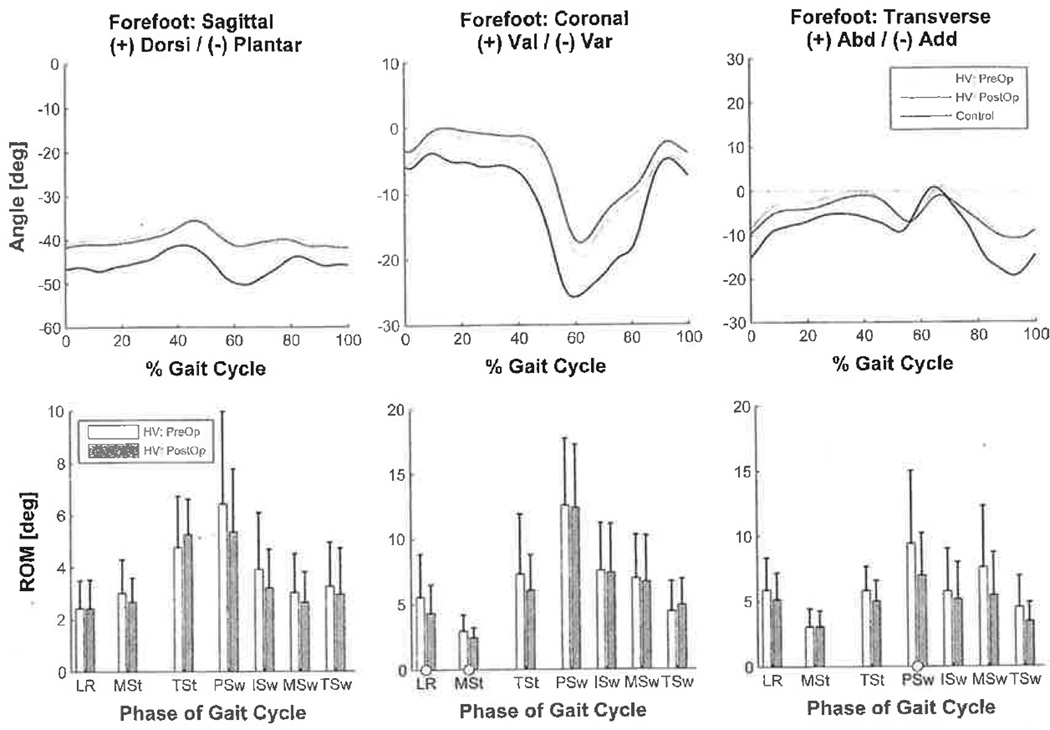
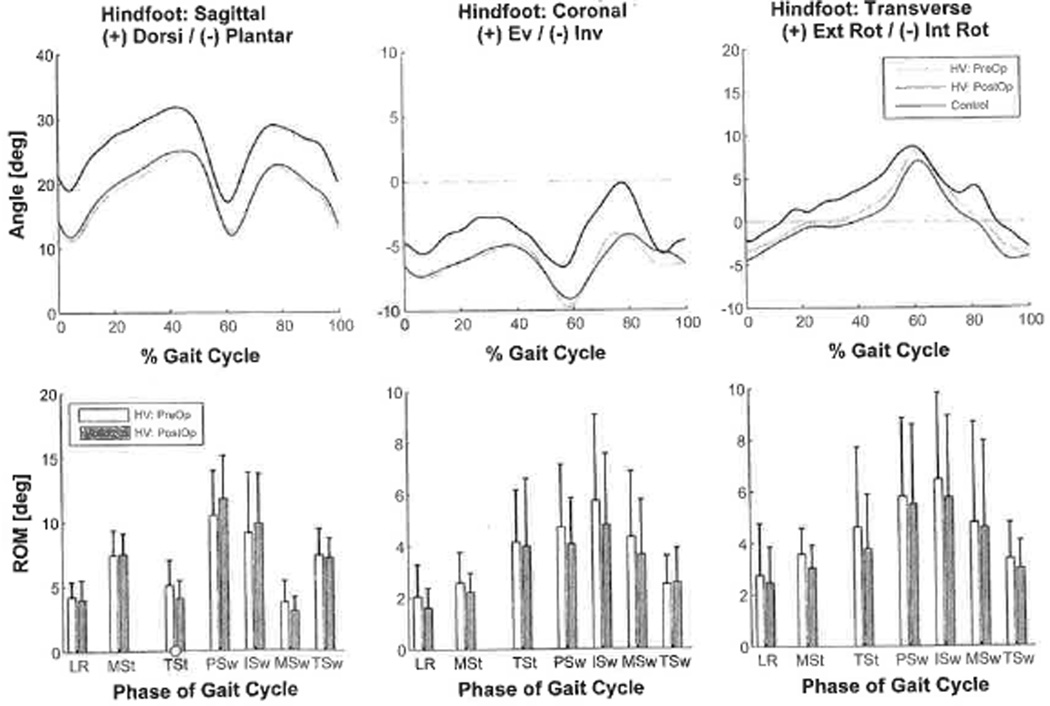
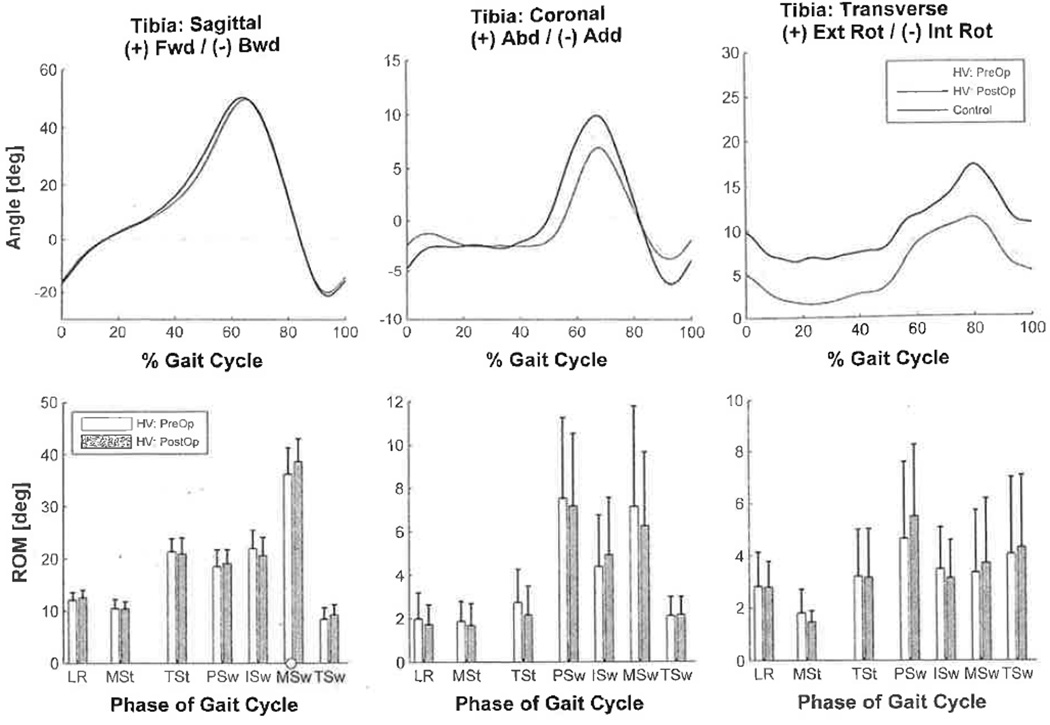
Results: Preoperatively, patients with hallux valgus showed significantly altered temporal-spatial and kinematic parameters. Postoperatively, kinematic analysis demonstrated restoration of hallux position to normal. Hallux valgus angles and intermetatarsal angles were significantly improved, and outcomes showed a significant increase in performance of physical activities. Temporal-spatial parameters and kinematics in the more proximal segments were not significantly changed postoperatively.
Conclusion: Postoperative results demonstrated significant improvement in foot geometry and hallux kinematics in the coronal and transverse planes. However, the analysis did not identify restoration of proximal kinematics.
Clinical relevance: Further investigation is necessary to explore possible causes/clinical relevance and appropriate treatment interventions for the persistently altered kinematics.
Figures
References
-
- Blomgren M, Turan I, Agadir M. Gait analysis in hallux valgus. J Foot Surg. 1991;30:70–71. - PubMed
-
- Bowling A, Bond M, Jenkinson C, Lamping DL. Short Form 36 (SF-36) Health Survey questionnaire: which normative data should be used? Comparisons between the norms provided by the Omnibus Survey in Britain, the Health Survey for England and the Oxford Healthy Life Survey. J. Public Health Med. 1999;21:255–270. http://dx.doi.org/10.1093/pubmed/21.3.255. - DOI - PubMed
-
- Brodsky JW, Beischer AD, Robinson AHN, Westra S, Negrine JP, Shabat S. Surgery for hallux valgus with proximal crescentic osteotomy causes variable postoperative pressure patterns. Clin Orthop. 2006;443:280–286. http://dx.doi.org/10.1097/01.blo.0000191269.50033.ec. - DOI - PubMed
-
- Buczek FL, Walker MR, Rainbow MJ, Cooney KM, Sanders JO. Impact of mediolateral segmentation on a multi-segment foot model. Gait Posture. 2006;23:519–522. http://dx.doi.Org/10.1016/j.gaitpost.2005.06.004. - DOI - PubMed
-
- Canseco K, Rankine L, Long J, et al. Motion of the multisegmental foot in hallux valgus. Foot Ankle Int. 2010;31:146–152. http://dx.doi.Org/10.3113/FAI.2010.0146. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
