

Effects of gestational age at birth on health outcomes at 3 and 5 years of age: population based cohort study
- PMID: 22381676
- PMCID: PMC3291750
- DOI: 10.1136/bmj.e896
Effects of gestational age at birth on health outcomes at 3 and 5 years of age: population based cohort study
Abstract
Objective: To investigate the burden of later disease associated with moderate/late preterm (32-36 weeks) and early term (37-38 weeks) birth.
Design: Secondary analysis of data from the Millennium Cohort Study (MCS).
Setting: Longitudinal study of infants born in the United Kingdom between 2000 and 2002.
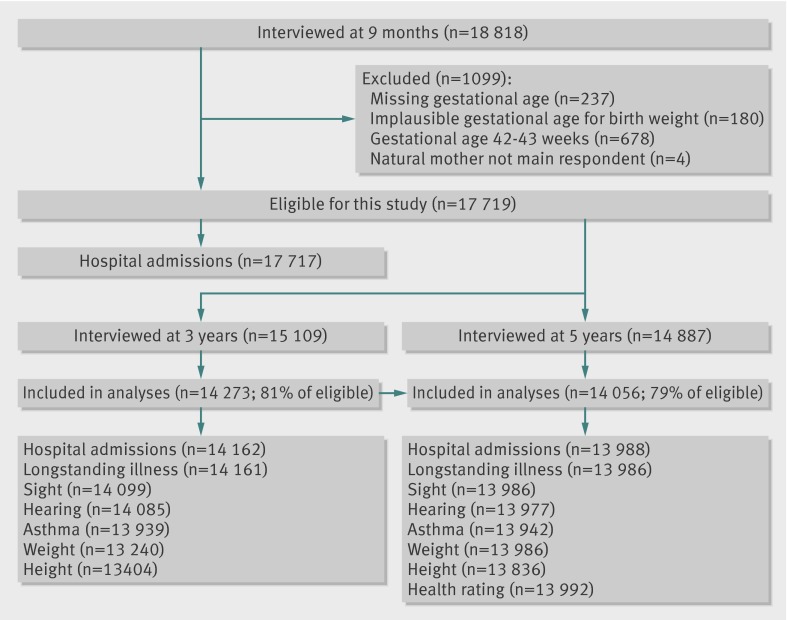
Participants: 18,818 infants participated in the MCS. Effects of gestational age at birth on health outcomes at 3 (n = 14,273) and 5 years (n = 14,056) of age were analysed.
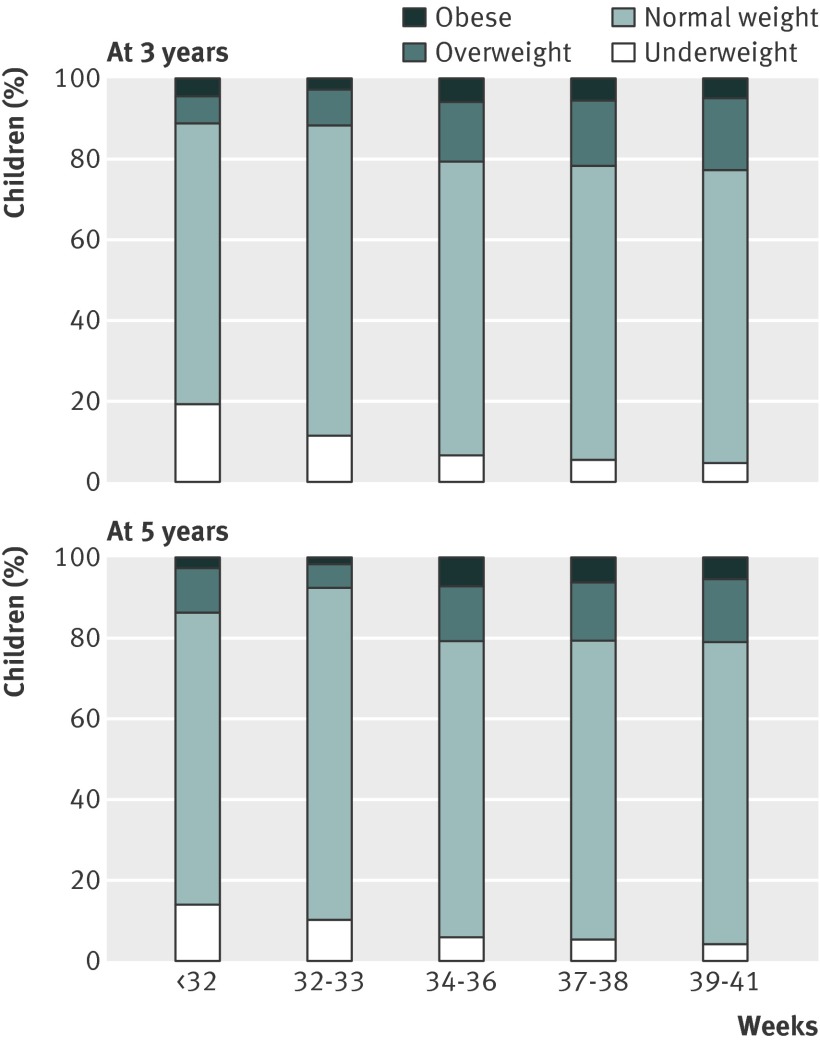
Main outcome measures: Growth, hospital admissions, longstanding illness/disability, wheezing/asthma, use of prescribed drugs, and parental rating of their children's health.
Results: Measures of general health, hospital admissions, and longstanding illness showed a gradient of increasing risk of poorer outcome with decreasing gestation, suggesting a "dose-response" effect of prematurity. The greatest contribution to disease burden at 3 and 5 years was in children born late/moderate preterm or early term. Population attributable fractions for having at least three hospital admissions between 9 months and 5 years were 5.7% (95% confidence interval 2.0% to 10.0%) for birth at 32-36 weeks and 7.2% (1.4% to 13.6%) for birth at 37-38 weeks, compared with 3.8% (1.3% to 6.5%) for children born very preterm (<32 weeks). Similarly, 2.7% (1.1% to 4.3%), 5.4% (2.4% to 8.6%), and 5.4% (0.7% to 10.5%) of limiting longstanding illness at 5 years were attributed to very preterm birth, moderate/late preterm birth, and early term birth.
Conclusions: These results suggest that health outcomes of moderate/late preterm and early term babies are worse than those of full term babies. Additional research should quantify how much of the effect is due to maternal/fetal complications rather than prematurity itself. Irrespective of the reason for preterm birth, large numbers of these babies present a greater burden on public health services than very preterm babies.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
References
-
- Wood NS, Marlow N, Costeloe K, Gibson AT, Wilkinson AR. Neurologic and developmental disability after extremely preterm birth. N Engl J Med 2000;343:378-84. - PubMed
-
- Moser K, Macfarlane A, Chow YH, Hilder L, Dattani N. Introducing new data on gestation-specific infant mortality among babies born in 2005 in England and Wales. Health Stat Q 2007;13:27. - PubMed
-
- Kramer MS, Demissie K, Yang H, Platt RW, Sauve R, Liston R. The contribution of mild and moderate preterm birth to infant mortality. JAMA 2000;284:843-9. - PubMed
-
- Tomashek KM, Shapiro-Mendoza CK, Davidoff MJ, Petrini JR. Differences in mortality between late-preterm and term singleton infants in the United States, 1995-2002. J Pediatr 2007;151:450-6,456.e1. - PubMed
-
- Escobar GJ, Clark RH, Greene JD. Short-term outcomes of infants born at 35 and 36 weeks’ gestation: we need to ask more questions. Semin Perinatol 2006;30:28-33. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical