

Screening and cervical cancer cure: population based cohort study
- PMID: 22381677
- PMCID: PMC3291751
- DOI: 10.1136/bmj.e900
Screening and cervical cancer cure: population based cohort study
Abstract
Objective: To determine whether detection of invasive cervical cancer by screening results in better prognosis or merely increases the lead time until death.
Design: Nationwide population based cohort study.
Setting: Sweden.
Participants: All 1230 women with cervical cancer diagnosed during 1999-2001 in Sweden prospectively followed up for an average of 8.5 years.
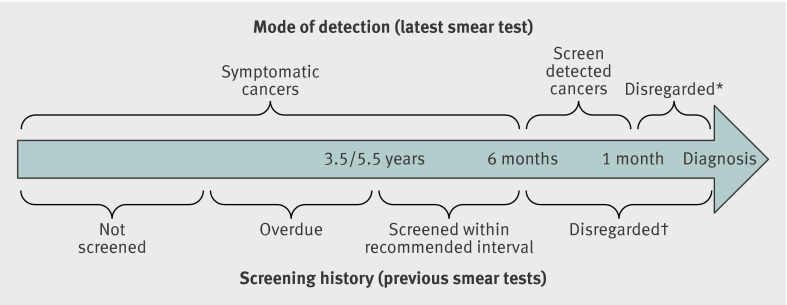
Main outcome measures: Cure proportions and five year relative survival ratios, stratified by screening history, mode of detection, age, histopathological type, and FIGO (International Federation of Gynecology and Obstetrics) stage.
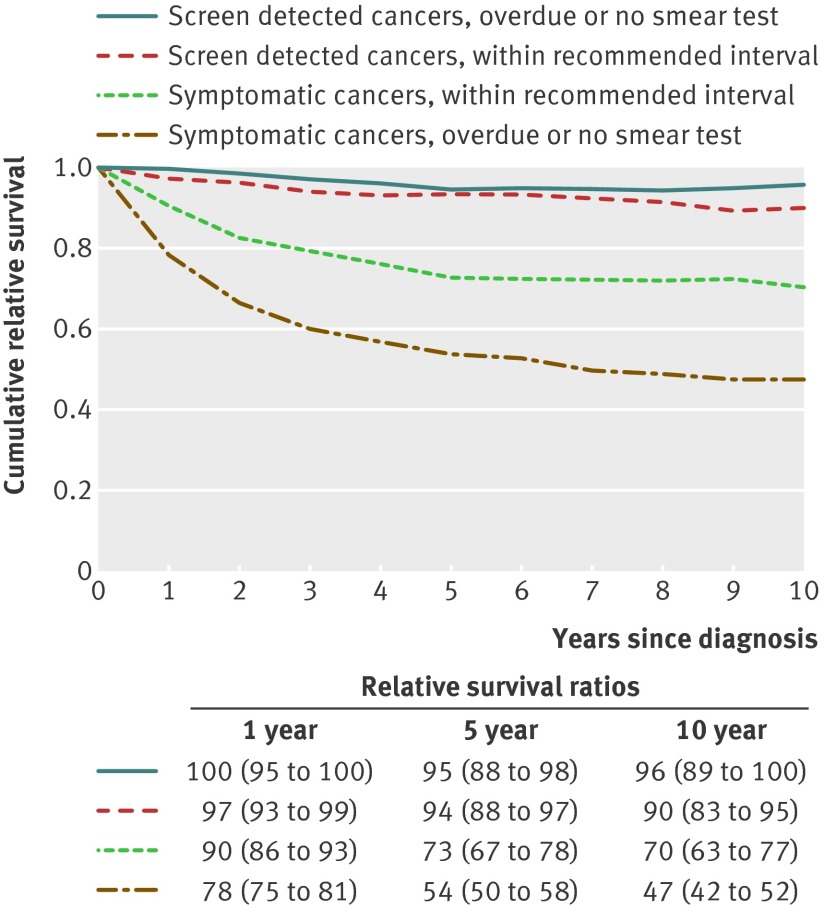
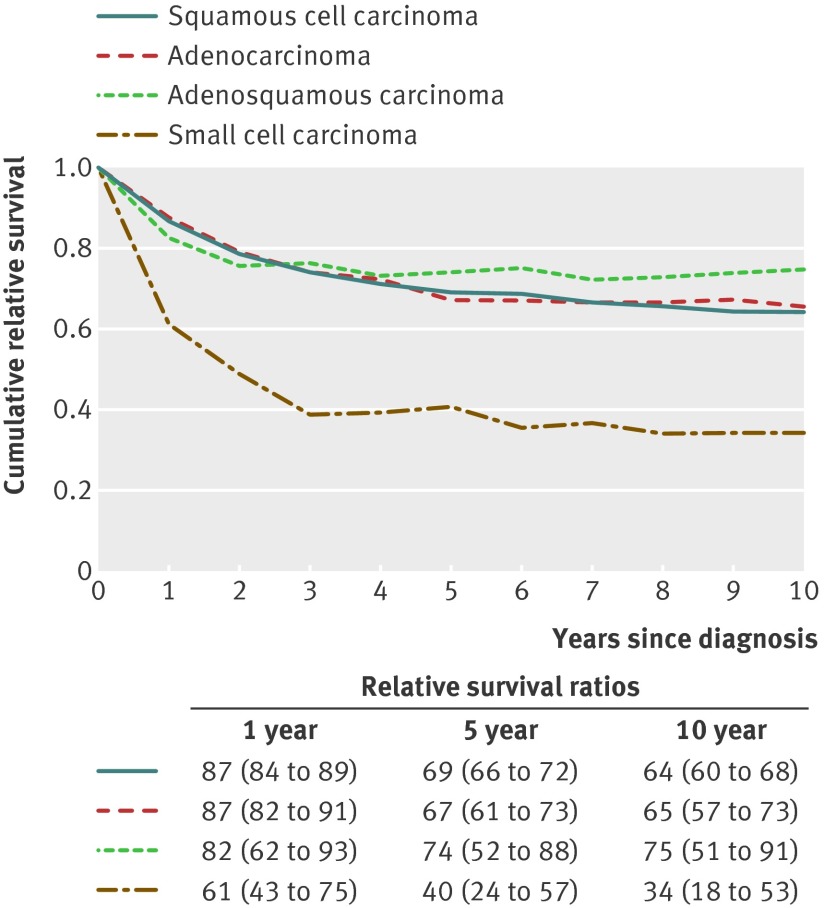
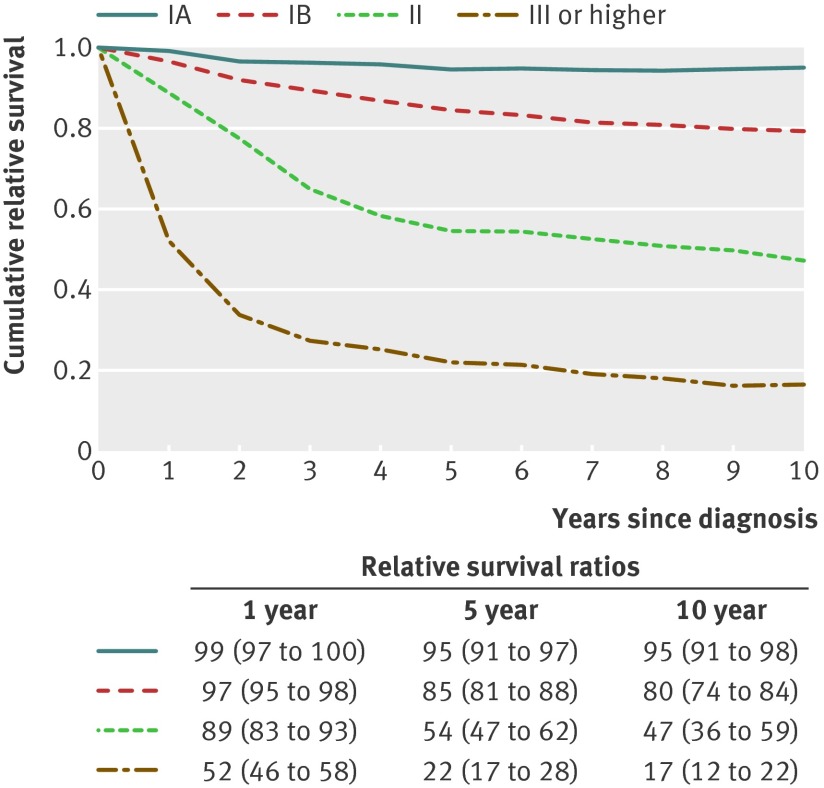
Results: In the screening ages, the cure proportion for women with screen detected invasive cancer was 92% (95% confidence interval 75% to 98%) and for symptomatic women was 66% (62% to 70%), a statistically significant difference in cure of 26% (16% to 36%). Among symptomatic women, the cure proportion was significantly higher for those who had been screened according to recommendations (interval cancers) than among those overdue for screening: difference in cure 14% (95% confidence interval 6% to 23%). Cure proportions were similar for all histopathological types except small cell carcinomas and were closely related to FIGO stage. A significantly higher cure proportion for screen detected cancers remained after adjustment for stage at diagnosis (difference 15%, 7% to 22%).
Conclusions: Screening is associated with improved cure of cervical cancer. Confounding cannot be ruled out, but the effect was not attributable to lead time bias and was larger than what is reflected by down-staging. Evaluations of screening programmes should consider the assessment of cure proportions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Effect of screening on deaths from cervical cancer in Sweden.BMJ. 2012 Mar 1;344:e804. doi: 10.1136/bmj.e804. BMJ. 2012. PMID: 22381675 No abstract available.
References
-
- Andrae B, Kemetli L, Sparen P, Silfverdal L, Strander B, Ryd W, et al. Screening-preventable cervical cancer risks: evidence from a nationwide audit in Sweden. J Natl Cancer Inst 2008;100:622-9. - PubMed
-
- Van der Aa MA, Schutter EM, Looijen-Salamon M, Martens JE, Siesling S. Differences in screening history, tumour characteristics and survival between women with screen-detected versus not screen-detected cervical cancer in the east of the Netherlands, 1992-2001. Eur J Obstet Gynecol Reprod Biol 2008;139:204-9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical