

Diagnosing Hunter syndrome in pediatric practice: practical considerations and common pitfalls
- PMID: 22383073
- PMCID: PMC3306562
- DOI: 10.1007/s00431-012-1703-y
Diagnosing Hunter syndrome in pediatric practice: practical considerations and common pitfalls
Abstract
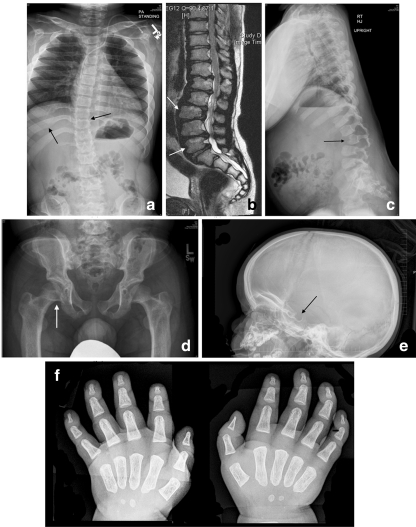
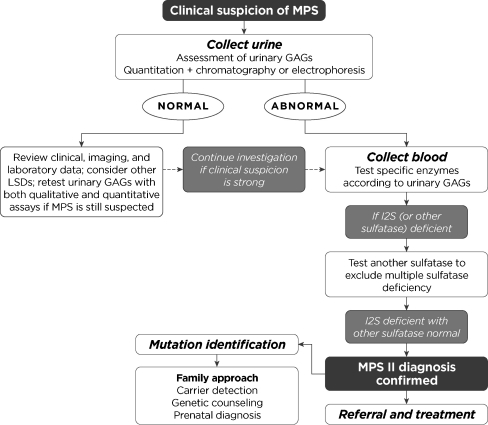
Mucopolysaccharidosis II (MPS II), or Hunter syndrome, is an X-linked lysosomal storage disorder caused by a deficiency in the enzyme iduronate-2-sulfatase. Affected patients suffer progressive damage to multiple organ systems and early mortality. Two thirds of patients also manifest cognitive impairment and developmental delays. MPS II can be extremely difficult to diagnose before irreversible organ and tissue damage has occurred because of an insidious onset and the overlap in signs and symptoms with common childhood complaints. This is particularly true of patients without cognitive impairment (attenuated phenotype). Although not curative, early treatment with enzyme replacement therapy before irreversible organ damage has occurred may result in the greatest clinical benefit. Here, the signs, symptoms, and surgical history that should trigger suspicion of MPS II are described, and the diagnostic process is reviewed with a focus on practical considerations and the avoidance of common diagnostic pitfalls. Once a diagnosis is made, multidisciplinary management with an extended team of pediatric specialists is essential and should involve the pediatrician or family practice physician as facilitator and medical home for the patient and family.
Conclusion: Because routine newborn screening is not yet available for MPS II, the involvement and awareness of pediatricians, family practice physicians, and pediatric specialists is critical for early identification, diagnosis, and referral in order to help optimize patient outcomes.
Figures


References
-
- Altarescu G, Renbaum P, Eldar-Geva T, Brooks B, Varshaver I, Avitzour M, Margalioth EJ, Levy-Lahad E, Elstein D, Epsztejn-Litman S, Eiges R (2011) Preventing mucopolysaccharidosis type II (Hunter syndrome): PGD and establishing a Hunter (46, XX) stem cell line. Prenat Diagn 31:853–860 - PubMed
-
- Chamoles NA, Blanco M, Gaggioli D. Diagnosis of alpha-L-iduronidase deficiency in dried blood spots on filter paper: the possibility of newborn diagnosis. Clin Chem. 2001;47:780–781. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
