

Acute myeloid leukemia in the real world: why population-based registries are needed
- PMID: 22383796
- PMCID: PMC3358248
- DOI: 10.1182/blood-2011-12-379008
Acute myeloid leukemia in the real world: why population-based registries are needed
Abstract
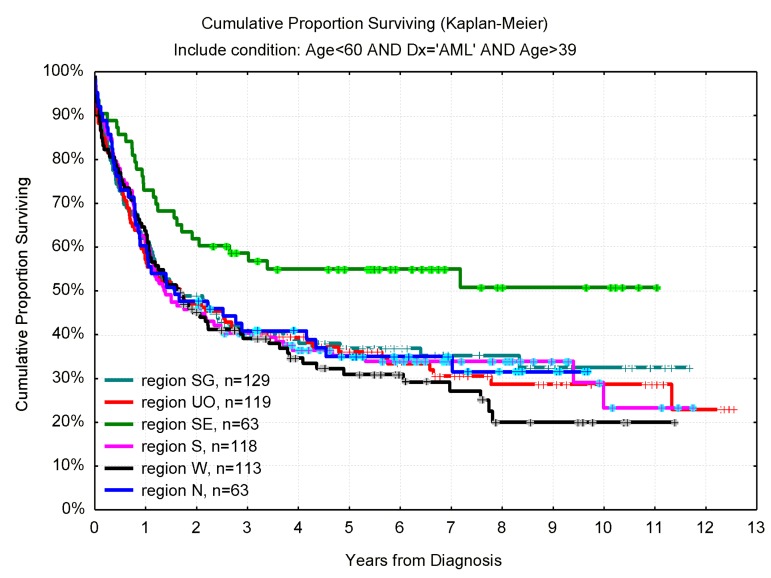
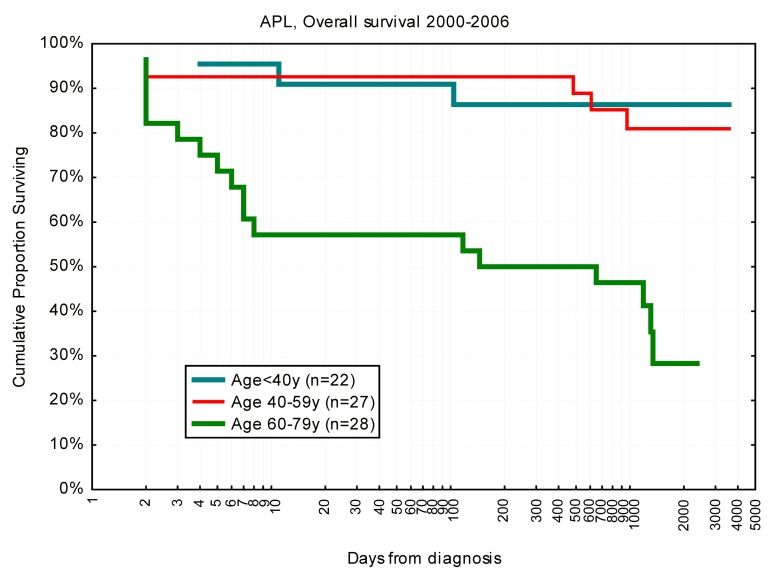
Population-based registries may provide data complementary to that from basic science and clinical intervention studies, all of which are essential for establishing recommendations for the management of patients in the real world. The same quality criteria apply for the evidence-based label, and both high representation and good data quality are crucial in registry studies. Registries with high coverage of the target population reduce the impact of selection on outcome and the subsequent problem with extrapolating data to nonstudied populations. Thus, data useful for clinical decision in situations not well covered by clinical studies can be provided. The potential clinical impact of data from population-based studies is exemplified with analyses from the Swedish Acute Leukemia Registry containing more than 3300 acute myeloid leukemia (AML) patients diagnosed between 1997 and 2006 with a median follow-up of 6.2 years on (1) the role of intensive combination chemotherapy for older patients with AML, (2) the impact of allogeneic stem cell transplantation on survival of younger patients with AML, and (3) the continuing problem with early deaths in acute promyelocytic leukemia. We also present the first Web-based dynamic graph showing the complex interaction between age, performance status, the proportion of patients given intensive treatment, early death rate, complete remission rate, use of allogeneic transplants, and overall survival in AML (non-AML).
Figures





References
-
- National quality registries in Sweden. 2011. [Accessed November 2011]. http://www.kvalitetsregister.se/om_kvalitetsregister/quality_registries.
-
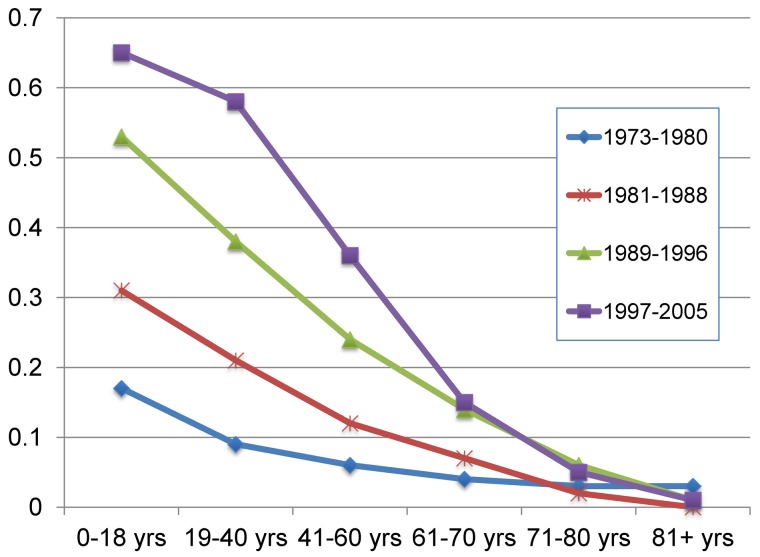
- Derolf AR, Kristinsson SY, Andersson TM, Landgren O, Dickman PW, Bjorkholm M. Improved patient survival for acute myeloid leukemia: a population-based study of 9729 patients diagnosed in Sweden between 1973 and 2005. Blood. 2009;113(16):3666–3672. - PubMed
